Conference: 07 - 2010 Case: 03 Lung - Cat
Signalment:
13-year-old, female, domestic long hair, feline (<i>Felis catus</i>).
Gross Description:
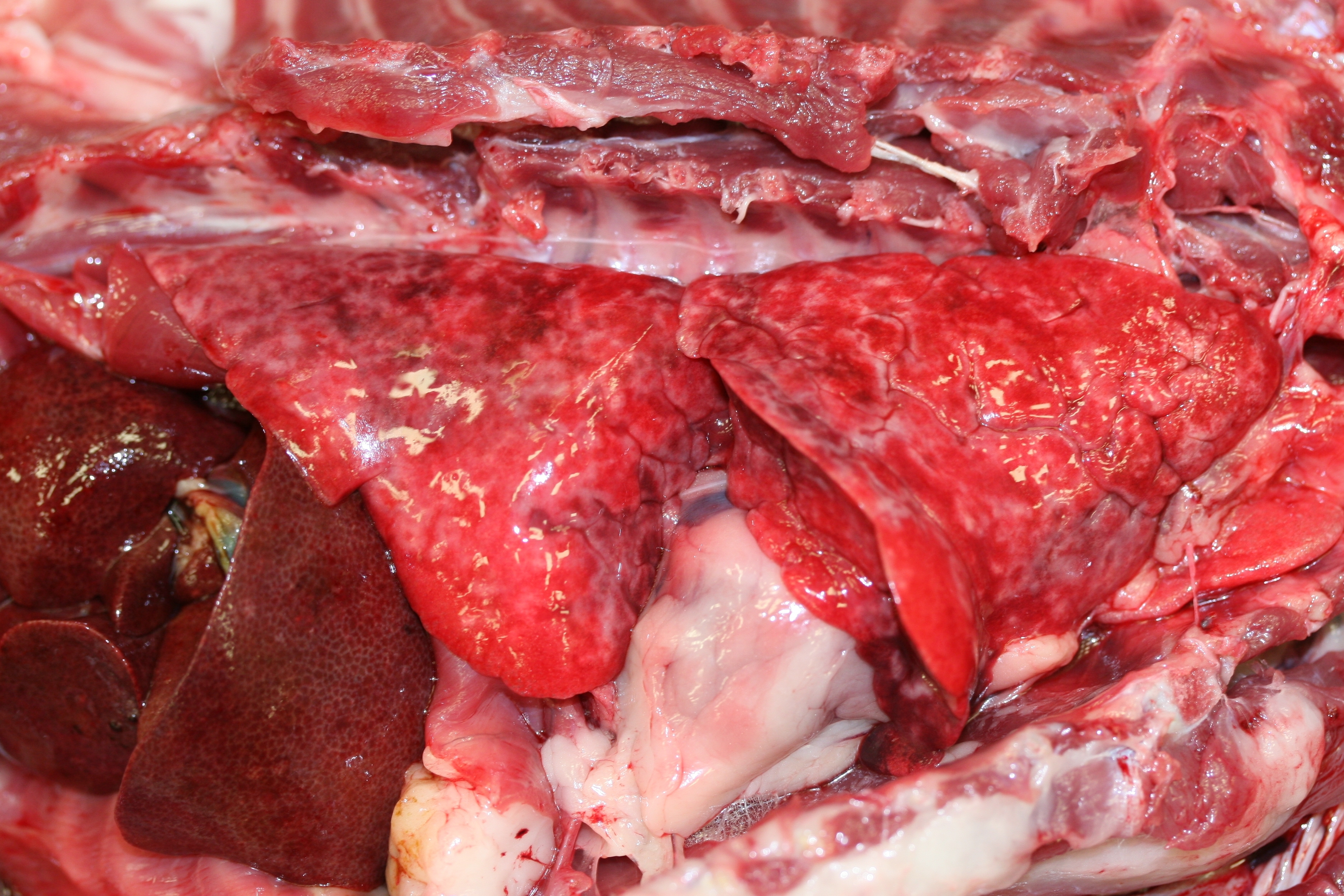
All lung lobes are diffusely firm, fail to collapse, and have an irregular surface that is mottled
pink and dark red (Fig. 2). The lungs ooze red fluid on cut section (edema).
History:
The cat had a 5-day history of increased respiration, with 3-4 days of rapid shallow breathing and 2 weeks
of weight loss. The owners had noticed a recent change in the cat's vocalization. Thoracic radiographs revealed a
diffuse bronchointerstitial pattern throughout the lungs (Fig. 1). There was no response to treatment with
bronchodilators or glucocorticoids.
Histopathologic Description:
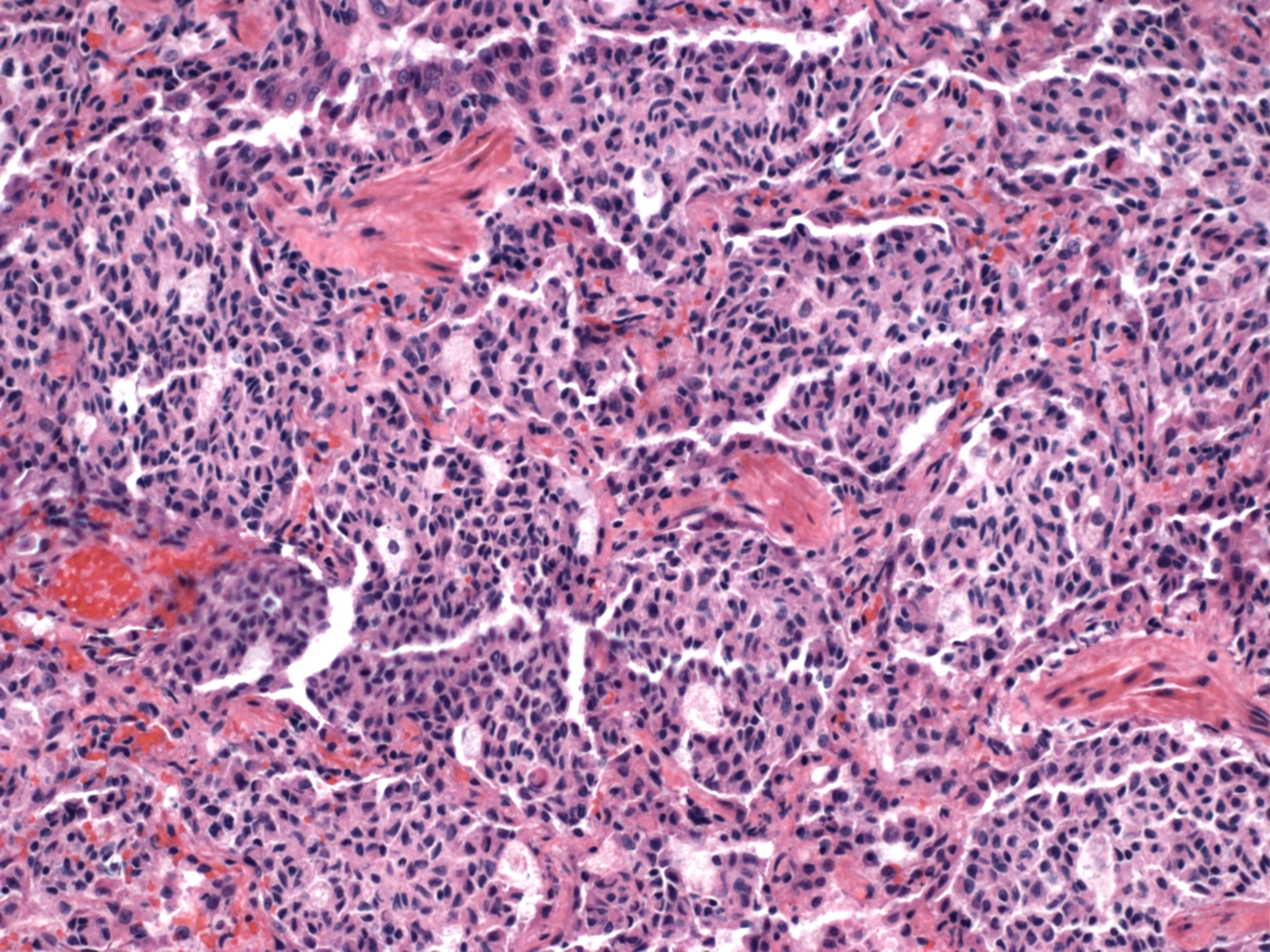
<u>Lung</u>: Throughout the section of lung, large numbers of alveoli and alveolar ducts
contain densely packed, round to slightly spindle-shaped cells with variably distinct cell borders that completely fill
the alveolar and ductal lumens. The cells form dense rounded clusters within alveoli and are often arranged in a
lightly streaming pattern. The infiltrating cells have a histiocytic appearance, characterized by a moderate amount of
lightly eosinophilic to pale basophilic cytoplasm, which is sometimes lightly vacuolated, and cell nuclei that are
round to oval, often eccentrically placed and slightly indented, and which contain variably condensed basophilic
chromatin. Mitotic figures are rare (<1 per 400x field). Some alveoli also contain individual or small central
clusters of macrophages with abundant, highly vacuolated, foamy cytoplasm and small condensed nuclei. Many
alveoli are segmentally lined by prominent, cuboidal epithelial cells (type II pneumocyte hyperplasia). The smooth
muscle within alveolar septae is markedly thickened in many areas (smooth muscle hyperplasia). Peribronchiolar
and peribronchial lymphocytes are prominent, and clusters of densely packed lymphocytes with lesser numbers of
plasma cells are also scattered throughout the section. Many alveoli contain abundant eosinophilic proteinaceous
fluid (edema). In some areas the normal alveolar architecture is replaced by thin interlacing bands of collagenous
tissue (interstitial fibrosis), with moderate numbers of lymphocytes and plasma cells and multifocal areas of mild
hemorrhage. Alveolar septae are lost in many areas resulting in enlarged, confluent air spaces (emphysema).
Morphologic Diagnosis:
Severe, diffuse, proliferative, alveolar histiocytosis with smooth muscle
hyperplasia, interstitial fibrosis and type II pneumocyte hyperplasia.
Lab Results:
Histoplasmosis antigen detection using an enzyme immunoassay was negative.
Condition:
Pulmonary Langerhans cell histiocytosis
Contributor Comment:
The marked pulmonary histiocytic disease in the lungs of this cat is representative of a
recently described histiocytic proliferative disorder in cats, pulmonary Langerhans cell histiocytosis (PLCH), that
targets the lungs but can variably affect other organs.(3) The severe bronchial pattern with a moderate interstitial
component observed throughout the lungs in thoracic radiographs of this cat (Fig. 1) was clinically suggestive of
histoplasmosis, severe asthma, or inflammatory airway disease. However, histoplasmosis antigen detection using an
enzyme immunoassay to detect antigenuria was negative, and the cat did not respond to treatment with
bronchodilators or glucocorticoids. Gross necropsy findings (Fig. 2), which included impression smears showing a
uniform population of what was presumed to be spindle cells, were more suggestive of pulmonary neoplasia or
fibrosis. The presence of a uniform population of cohesive and streaming histiocytic cells within many alveoli and
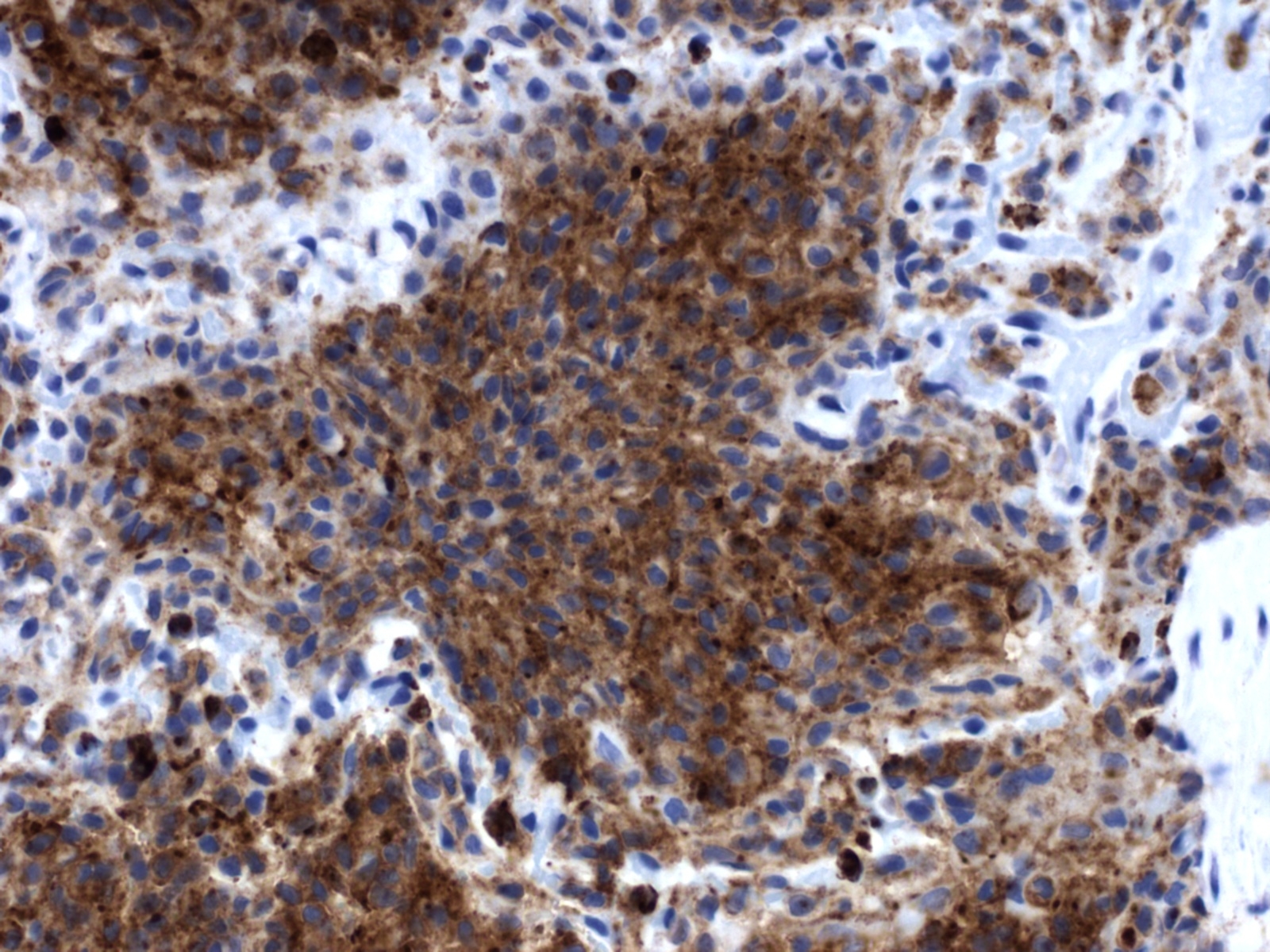
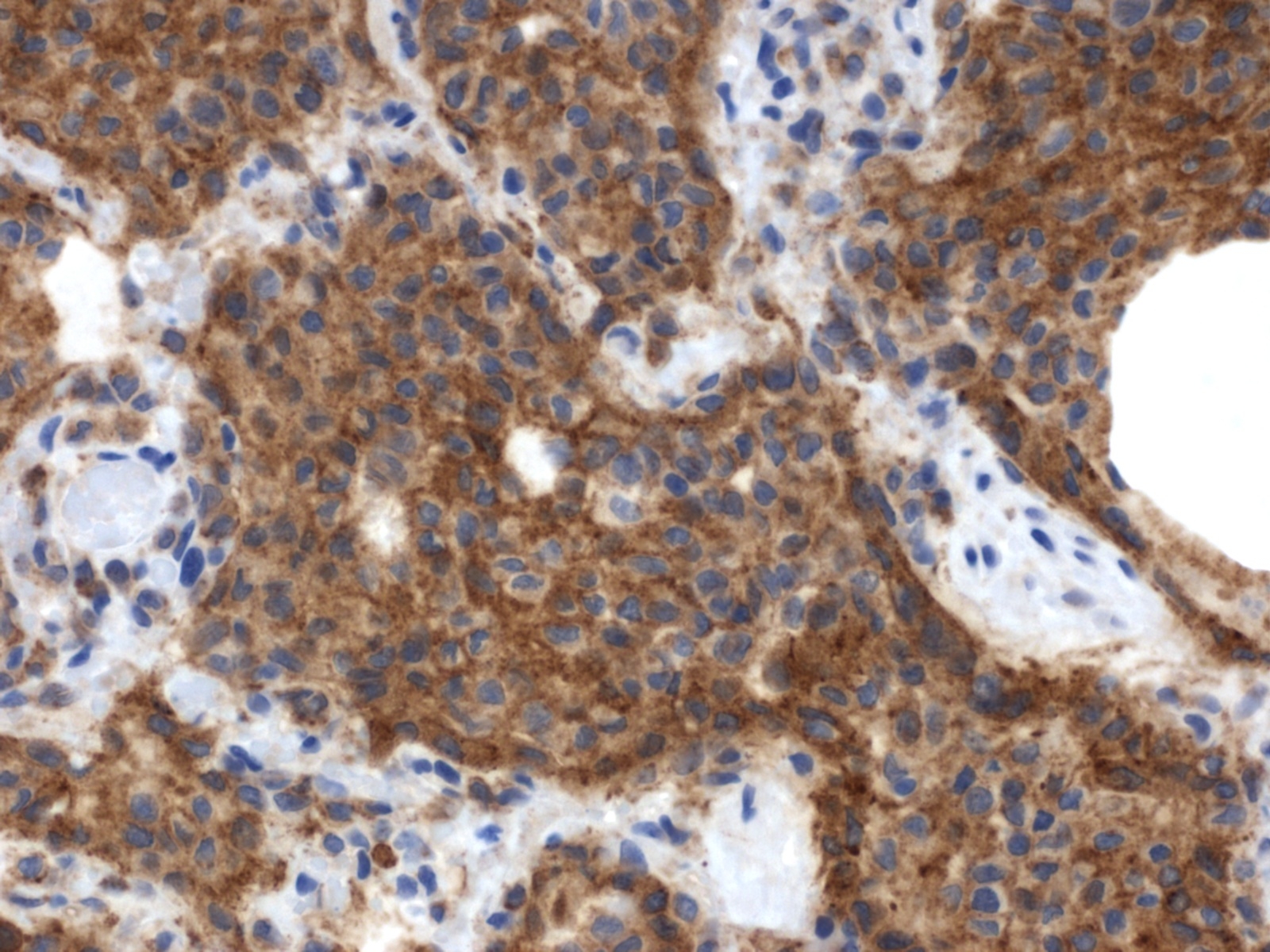
alveolar ducts throughout the lung of this cat is consistent with PLCH (Fig. 3). The infiltrating cells were strongly
positive for vimentin, CD18 (Fig. 4), and E-cadherin (Fig. 5), which supports a Langerhans cell phenotype as
previously described.(3)
<br><br>
In the corresponding human interstitial lung disease, which occurs primarily in young adult cigarette smokers,
PLCH was found to be the result of mixed clonal and nonclonal expansion of nonmalignant Langerhans cells that
arises in a setting of Langerhans cell hyperplasia.(11) This, along with the fact that it is frequently associated with
clinical regression after steroid therapy and cessation of smoking, supports the view that PLCH represents a reactive
disorder rather than a neoplastic process. It occurs in a slightly higher percentage in women and is frequently found
only in the lungs, although multiorgan involvement may also occur.(9,10) PLCH represents one of a spectrum of
Langerhans cell proliferative diseases (Langerhans cell histiocytosis), which occur more frequently in children and
are marked by proliferation and infiltration of various organs by Langerhans cells.(8,10) In addition to the lung, the
organs most commonly affected by Langerhans cell histiocytosis include bone and skin, although any organ can be
affected. In the recent report of PLCH in 3 cats, affected organs included the lung, pancreas, kidney, liver, and
various lymph nodes.(3) Extrapulmonary involvement was not observed in the present case. A characteristic feature
of PLCH, in addition to the marked proliferation of alveolar histiocytes, is the presence of rod-shaped Birbeck
granules, the hallmark organelle of the Langerhans cell, within the cytoplasm of lesional histiocytes when viewed
with transmission electron microscopy.
JPC Diagnosis:
Lung: Histiocytosis, atypical, intrabronchiolar and intra-alveolar, multifocal, marked, with
extensive alveolar edema, moderate lymphoplasmacytic and histiocytic inflammation, and hyperplasia of
bronchiolar smooth muscle, consistent with pulmonary Langerhans cell histiocytosis.
Conference Comment:
Conference participants readily identified the overwhelming infiltrate of histiocytic cells in
the lung described by the contributor, but most experienced difficulty with histologic interpretation of the underlying
pathologic process; some favored a neoplastic condition, while others interpreted the lesion as granulomatous
inflammation. The conference moderator emphasized that the infiltrative cell type consists almost exclusively of
histiocytic cells with mildly atypical morphology, including mild anisokaryosis and hyperchromatic nuclei,
supporting a histiocytic proliferative lesion versus granulomatous inflammation. The striking similarity to the cases
reported by Busch et al. strongly supports pulmonary Langerhans cell histiocytosis (PLCH). The
immunohistochemical findings reported by the contributor provide further confirmation.
<br><br>
Reports of histiocytic diseases of the cat are few and limited to feline progressive histiocytosis,2 feline pulmonary
Langerhans histiocytosis,(3) histiocytic sarcoma(7) and hemophagocytic histiocytic sarcoma;(4) the cell type in the first
two conditions is of Langerhans cell lineage, dendritic cell origin for the third while the findings in the last entity are
most consistent with macrophage origin. In the feline progressive histiocytosis and feline pulmonary Langerhans
histiocytosis, it remains uncertain whether the conditions represent a reactive or neoplastic process. In contrast to
cats, histiocytic diseases in the dog are much more common, and the nature of the conditions as reactive or
neoplastic are better characterized. The classifications and corresponding cell of origin are as follows: reactive
cutaneous/systemic histiocytosis (interstitial dendritic cell); cutaneous histiocytoma (Langerhans cell); local and
disseminated histiocytic sarcoma (myeloid dendritic cell); and hemophagocytic histiocytic sarcoma (macrophage).
(1,5,7)
<br><br>
Development of dendritic cells, Langerhans cells and macrophages begins with CD34+ progenitor cells in the bone
marrow, and further differentiation produces three subsets of cells: CD34+/CLA+ (cutaneous lymphocyte antigen);
CD34+/CLA-; and CD34+/IL-3Rα-rich cells.(1) The CD34+/CLA+ and CD34+/CLA- cells, under the influence of
stem cell factors (GM-CSF and TNF-α) differentiate into CD1+/CD14- and CD1a-/CD14+ cells, respectively.
Again, under the influence of GM-CSF and TNF-α, CD1a-/CD14+ cells differentiate into interstitial dendritic cells,
or, if stimulated by M-CSF, undergo differentiation to macrophages. The CD1+/CD14- subtypes differentiate into
Langerhans cells under the influence of GM-CSF, TNF-α, and TGF-β. The CD1a/CD14+ subtypes can also arise
from CD14+ blood monocytes under the influence of GM-CSF and IL-4. Myeloid dendritic cells arise from CD34
+/IL-3Rα-rich cells when stimulated by IL-3 and GM-CSF.(1)
<br><br>
The immunophenotyping of the cells comprising the histiocytic diseases varies based on the reference text or journal
consulted, and reflects the continuous information explosion in this very active field of research. After review of the
literature and the veterinary reference text of Jubb, Kennedy and Palmers Pathology of Domestic Animals, the
following list outlines the most consistent and commonly cited immunophenotypes:(1-7)
<ul>
<li> Langerhans cells: MHC II; CD1a, c; CD11c; CD18; langerin; ICAM-1; and E-cadherin positive
<li> Interstitial dendritic cells: MHC II; CD1c; CD4; CD11b, c; CD18; CD90 (Thy-1) positive
<li> Myeloid dendritic cells: MHC II; CD1; CD11c; ICAM-1; -� CD90 positive
<li> Macrophage: MHC II; CD11d/CD18; β2-integrin; -� CD11c/CD18 and CD1c positive
</ul>
<br><br>
Readers are encouraged to review <a href="http://vp4.afip.org/wsco/wsc_showconference.php?id=208"><font color="blue">Wednesday Slide Conference 24, Case IV, 2008-2009</font></a>, for a thorough review of
canine histiocytic diseases.
References:
1. Affolter VK, Moore PF. Localized and disseminated histiocytic sarcoma of dendritic cell origin in dogs. <i>Vet
Pathol</i>. 2002;39:74-83.
<br>
2. Affolter VK, Moore PF. Feline progressive histiocytosis. <i>Vet Pathol</i>. 2006;43:646-655.
<br>
3. Busch MDM, Reily CM, Luff JA, Moore PF. Feline pulmonary Langerhans cell histiocytosis with multiorgan
involvement. <i>Vet Pathol</i>. 2008;45(6):816-824.
<br>
4. Friedrichs KR, Young KM. Histiocytic sarcoma of macrophage origin in a cat: case report with a literature review
of feline histiocytic malignancies and comparison with canine hemophagocytic histiocytic sarcoma. <i>Vet Clin
Pathol</i>. 2008;37(1):121-128.
<br>
5. Fulmer AK, Mauldin GE. Canine histiocytic neoplasia: an overview. <i>Can Vet J</i>. 2007;48:1041-1050.
<br>
6. Ginn PE, Mansell JEKL, Rakich PM. Skin and appendages. In: Maxie MG, ed. <i>Jubb, Kennedy and Palmers
Pathology of Domestic Animals</i>. 5th ed., vol. 1. Philadelphia, PA: Elsevier Ltd; 2007:768-770.
<br>
7. Gross TL, Ihrke PJ, Walder EJ, Affolter VK. Histiocytic Sarcoma. In: <i>Skin diseases of the dog and cat, clinical
and histopathologic diagnosis</i>. 2nd ed., Ames, Iowa: Blackwell Science Ltd; 2005:848-852.
<br>
8. Moore PF, Affolter VK, Vernau W. Canine hemophagocytic histiocytic sarcoma: a proliferative disorder of
CD11d+ macrophages. <i>Vet Pathol</i>. 2006:43:632-645.
<br>
9. Satter, EK. High WA. Langerhans cell histiocytosis: a review of the current recommendations of the histiocyte
society. <i>Pediatr Dermatol</i>. 2008;25(3)291-295.
<br>
10.Vassalo, R, Ryu JH. Pulmonary Langerhans cell histiocytosis. <i>Clin Chest Med</i>. 2004;25(3):561-571.
<br>
11.Vassalo, R, Ryu, JH, Colby TV, et al. Pulmonary Langerhans-cell histiocytosis. <i>N Engl J Med</i>. 2000;342(26):
1969-1978.
<br>
12.Yousem SA, Colby TV, Chen YY, et al. Pulmonary Langerhans cell histiocytosis: molecular analysis of clonality.
<i>Am J Surg Pathol</i>. 2001;25(5):630-636.3.