Conference 24
CASE II:
Signalment:
Cat, domestic shorthair, 12 years-old, neutered male.
History: The cat was euthanized and the body was transferred to the necropsy service without any medical history.
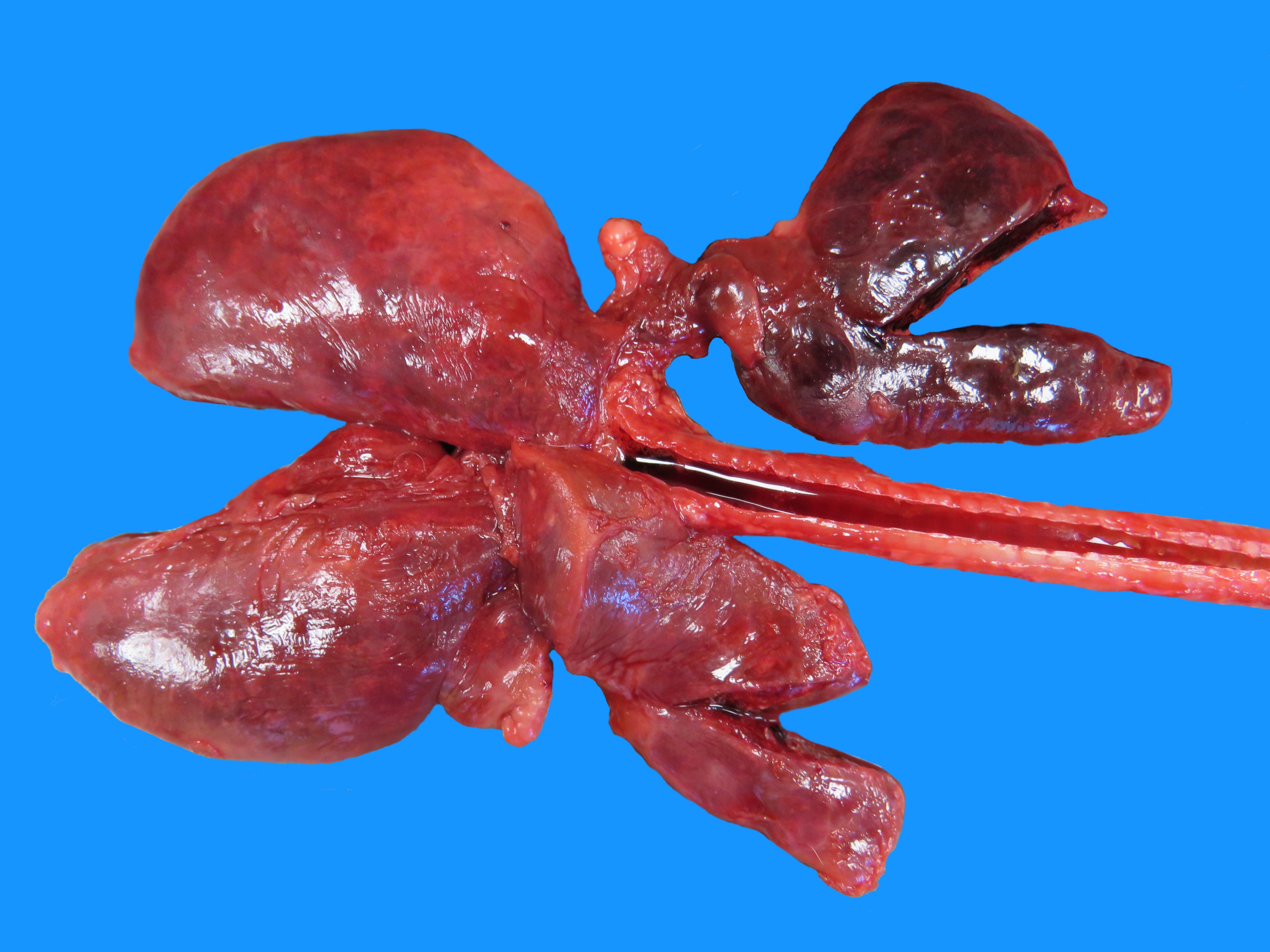
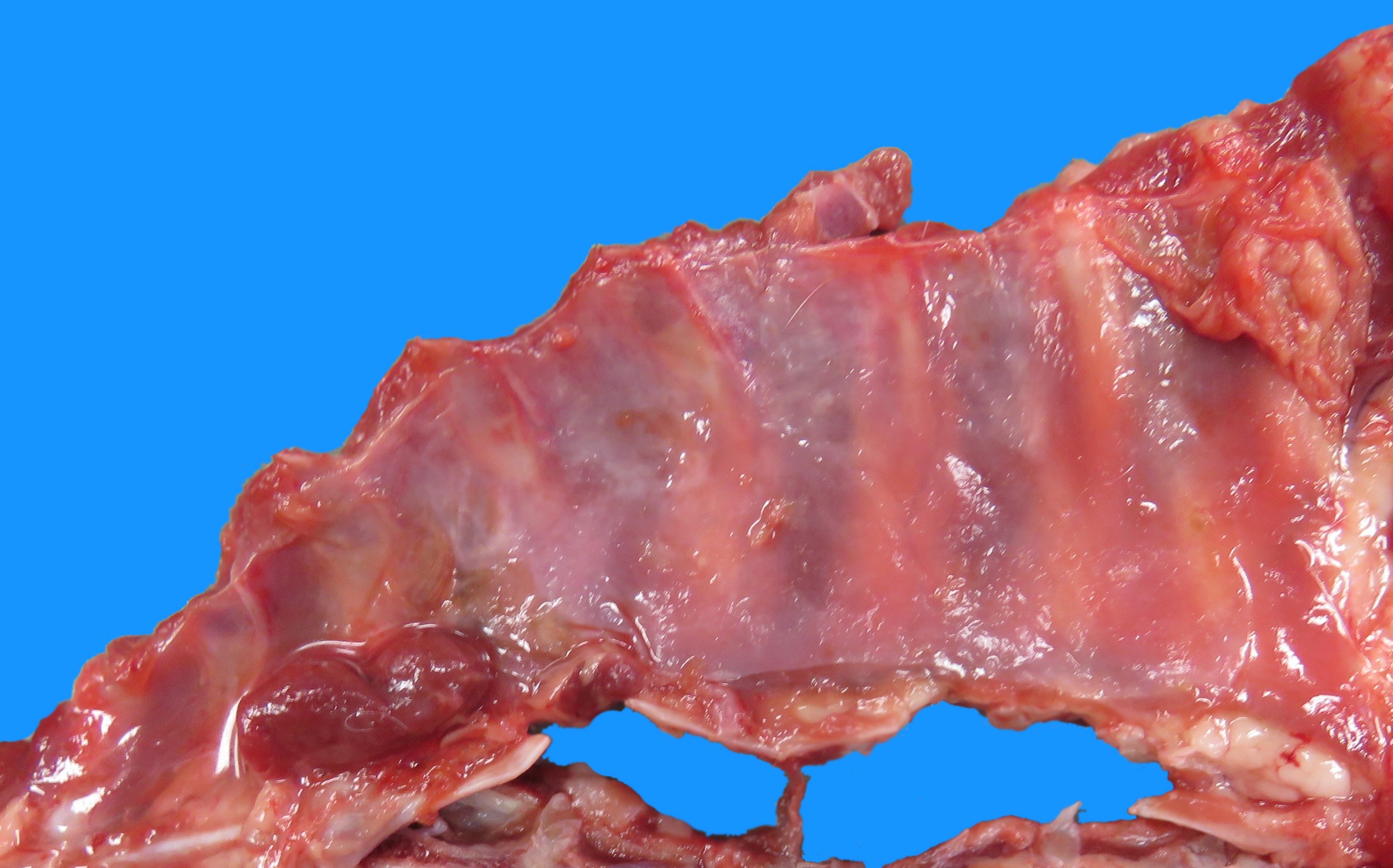
Gross Pathology: The body was well preserved. The animal was in good body condition with abundant fat. About 150 ml of a latescent thoracic effusion (suspected chylous effusion) was present and associated to a white diffuse and moderate thickening of the pleura with occasional strands of fibrin (suspected chronic fibrosing pleuritis, fig 1). No obvious cardiac anomaly was observed but alterations due to euthanasia with barbiturates prevented an optimal gross examination of the heart. Pulmonary lobes were slightly rounded and had a slightly thickened pleura. The left cranial pulmonary lobe was twisted at approximatively 180° around its hilus (lung lobe torsion), and was markedly and diffusely red, with blood oozing after sectioning (venous infarction).
Other organs did not show significant gross lesions.
Laboratory Results:
Cytological analysis of the effusion was performed:
gross aspect: lactescent (persistent after centrifugation)
cellularity: 1380 nucleated cells per mm3;
protein concentration: 45 g/l (determined by refractometry)
cells: numerous small lymphocytes and fewer foamy macrophages and neutrophils. No neoplastic cells or infectious agent were identified.
In cats, these findings are suggestive of a chylous effusion and/or an effusion secondary to cardiac insufficiency (although no gross cardiac anomaly was observed). Cholesterol and triglycerides concentrations were not assessed.
Microscopic Description:
Heart (not submitted): No significant histological findings
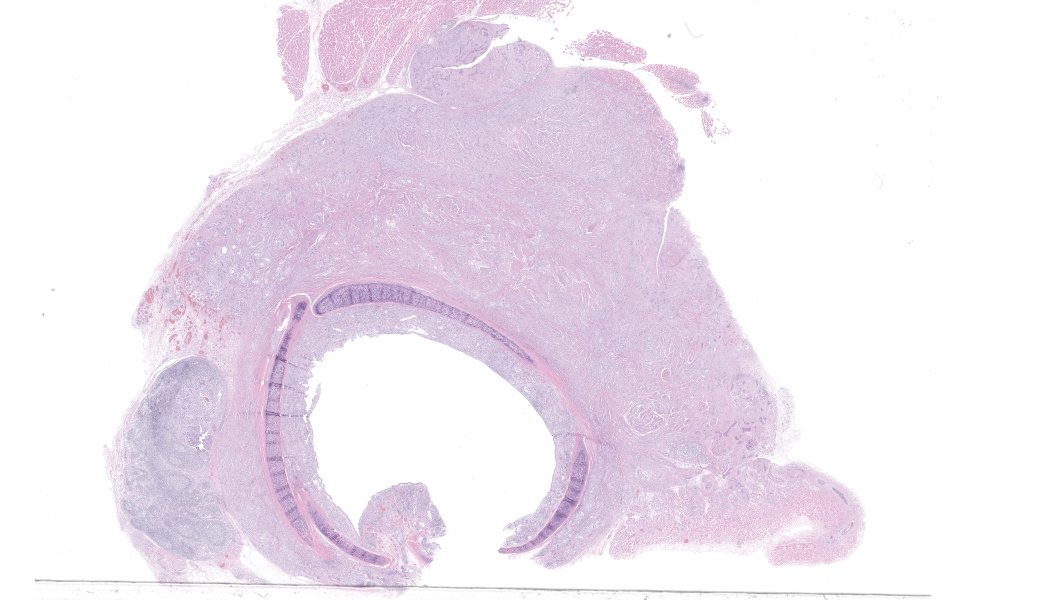
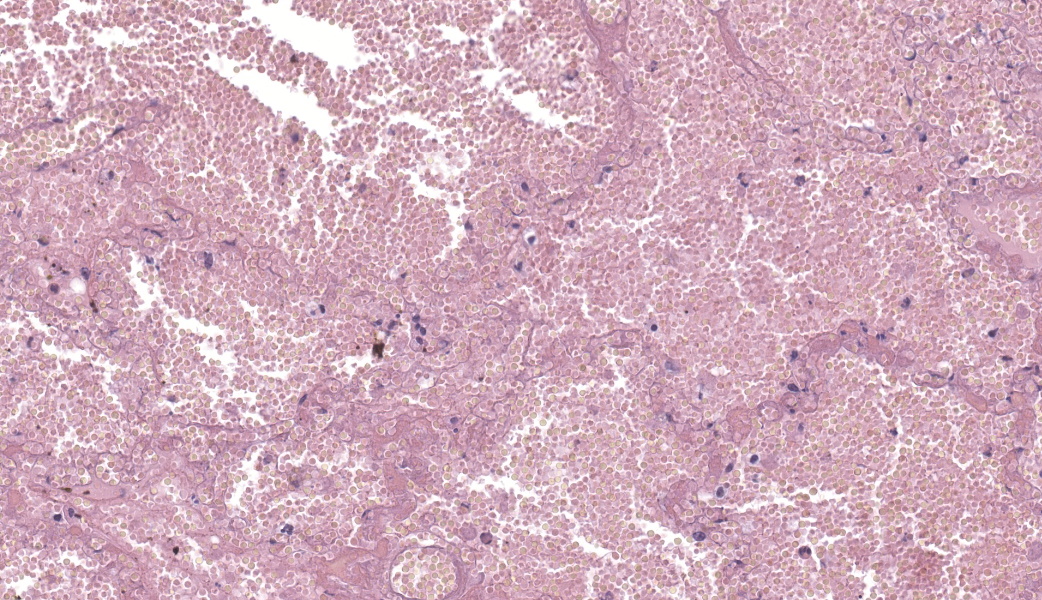
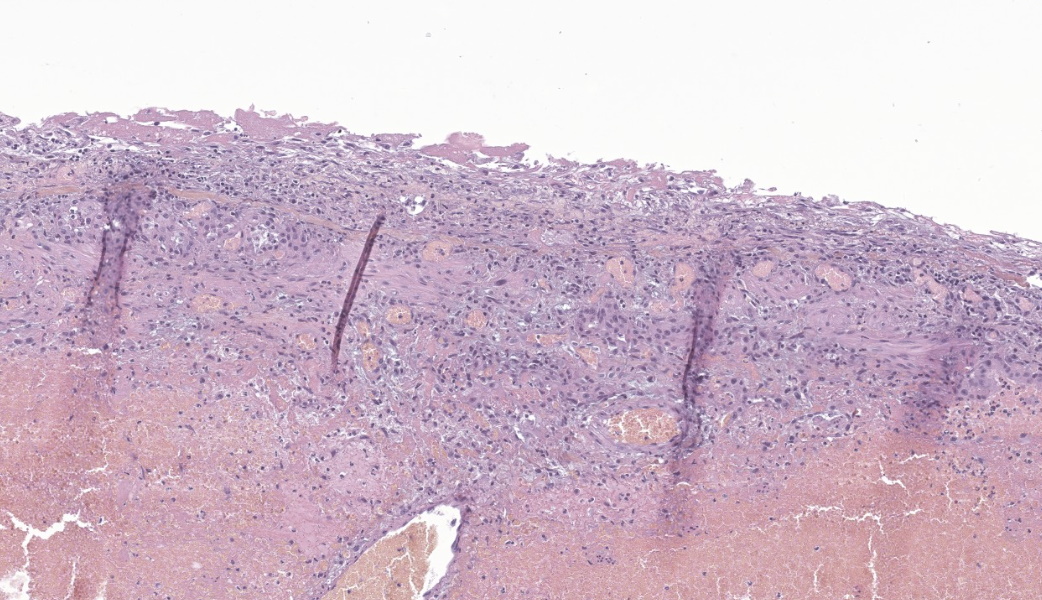
Lungs: Three sections are submitted. Two are from the left cranial lobe (twisted lobe), the third one is from the left caudal lobe. Sections from the left cranial lobe show extensive and severe alveolar hemorrhages and marked vascular congestion. Alveolar walls are often diffusely eosinophilic with loss of basophilia (necrosis).
The left caudal lobe section shows occasional foci of fibrin exudation within the alveoli.
All three sections show a moderate to marked thickening of the pleura by a fibrovascular tissue, resembling granulation tissue, containing a variable amount of mature collagen and occasionally covered with fibrin. The underlying pleural tissue shows a slight to moderate infiltration with lymphocytes.
Prussian blue stain is negative on all sections.
Contributor's Morphologic Diagnosis:
Lungs :
Left cranial lobe: acute, severe, diffuse hemorrhagic necrosis (venous infarction) secondary to lobe torsion
Left caudal lobe: acute, minimal, multifocal, fibrinous alveolitis
Left cranial and caudal lobes: Chronic, moderate to marked, diffuse fibrinous and fibrosing pleuritis
Contributor's Comment: This case is a nice example of lung lobe torsion secondary to a chylothorax. Chylous effusions are composed of chyle. Chyle is a chylomicron-rich lymph fluid originating from the intestinal lacteals and circulating through the intestinal and mesenteric lymphatic vessels, the cisterna chyli and the thoracic duct that ultimately terminates in the left external jugular vein or jugulo-subclavian angle.10,14 Chyle has a typical opaque white, milky (lactescent) to slightly pink color that persists after centrifugation. Cytologically, it is mainly composed of small lymphocytes and fewer foamy macrophages. Neutrophils may be present following repeated thoracocenteses. Chylous effusion can be confirmed biochemically by measurement of triglycerides and cholesterol concentrations in the effusion and in the serum: triglyceride concentration is typically higher in the effusion compared to serum, whereas the reverse is true for cholesterol concentration.14
The majority of chylous effusions are in the thorax (chylothorax). Most chylothorax are idiopathic, as suspected in this case.10,14 Known causes of chylothorax are traumatic rupture of the thoracic duct, cardiomyopathy, right-sided heart failure, vena caval thrombosis, heart worms (dirofilariasis), thoracic neoplasia (thymoma, lymphoma, lymphangiosarcoma) or inflammatory lesions that cause obstruction of the thoracic duct.6,10,14 Lung lobe torsion is also reported to cause chylothorax although the real sequence of events is not always clear in affected animals (see later).12,14 Chyloabdomen is much less common than chylothorax. A study reported that almost half of chyloabdomens in dogs and cats occur in association with chylothorax and that in these cases the most common underlying cause is neoplasia.5
Although chyle is considered to be non-irritant, chronic chylothorax may lead to pleural fibrosis (fibrosing pleuritis), especially in cats, as illustrated in this case.2,13,14 Macroscopically, lungs may be shrunken, rounded, and covered by a thick pleura.2 This may lead to reduced pulmonary expansion and dyspnea even with minimal residual effusion.2,10
In lung lobe torsion, affected lobes are deeply congested due to compression of veins at the site of torsion, preventing blood return to the heart and leading to severe congestion, hemorrhages and necrosis (venous infarction).9 The compression does not affect arteries that have a thicker wall and higher hydrostatic pressure. As a consequence, blood may still penetrate the tissue.
The treatment of choice for lung lobe torsion is surgery after medical stabilization of the animal. Of note, the affected lobe should not be untwisted in order to avoid the release by hypoxic tissues of inflammatory cytokines, endotoxins, hypoxanthine and free radicals, as in the phenomenon of ischemia-reperfusion.3,8,9
Pleural effusion is often present in association with lung lobe torsion.10,12,14 The effusion varies in nature (transudate, chyle, exudate, blood). There seems to be a debate regarding the pathogenesis of these effusions because some consider it to be a cause while others see it as a consequence of the lobe torsion.8,12,14 Both cases might happen. In the present case, the lung torsion appears to be a recent event based on the lack of hemosiderin in the hemorrhagic parenchyma. On the contrary, the fibrosing pleuritis suggests that the chylothorax is chronic and should therefore be considered as the most likely cause for the lung lobe torsion in this cat.
Torsions can affect other organs such as hepatic lobes (pigs, cats, dogs, horses, rabbits), testes (horses, dogs), urinary bladder (dogs), uterus (especially in mares and cows) and caecum (cattle).4,14 Hepatic lobe torsion has recently been described in three dromedary camels.7
Contributing Institution:
Unite d'Histologie et d'Anatomie pathologique, Ecole Nationale veterinaire d'Alfort (EnvA). France www.vet-alfort.fr
JPC Morphologic Diagnosis:
- Lung: Alveolar necrosis and hemorrhage, regionally extensive, severe (lobar torsion).
- Lung, pleura: Pleuritis, fibrosing, chronic-active, diffuse, moderate.
JPC Comment:
The WSC has not seen a lung lobe torsion case since 1983! This second case also proved challenging and resulted in a variety of diagnoses from participants. There were some features on the slide that contributed to the confusion, including a lack of thrombosis, very little inflammation, and minimal fibrin within the lung coupled with significant edema and pleural changes (mesothelial hyperplasia, fibrosis, and fibrin). The primary supporting finding for the diagnosis of lung lobe torsion was the abundant congestion, intra-alveolar hemorrhage, and multifocal septal necrosis. The pleural changes threw participants for a loop when settling on a diagnosis. The changes were indicative of an acute-on-chronic process which, as mentioned by the contributor in their write-up, can occur with chronic chylothorax.2,13,14 However, another primary cause for pleuritis in cats that was not tested for in this particular case is feline infectious peritonitis (FIP).1 Although there were other features of FIP lacking in this case, it is always something to keep on the differential list for cases of pleural effusion of any kind in feline patients.1
A crucial contributor to the pathogenesis of lung lobe torsions is the dual blood supply to the lung, which has low and high-pressure systems. The pulmonary circulation, the low-pressure system, is where gas exchange occurs in the lung.11 The bronchiolar circulation is the high-pressure system responsible for providing oxygen to the lung tissue itself.11 When a lung lobe torsion occurs, the low-pressure system collapses, leading to venous infarction and coagulative necrosis of the alveoli.9 The high-pressure system continues to pump oxygenated blood, leaving the bronchioles relatively intact.
Dr. Carvallo wrapped up this case with a discussion on a rarely mentioned topic in the lungs: the lymphatic circulation.9 The lung does have a significant lymphatic network that drains from the interstitium to the mediastinal lymph nodes and back into the venous circulation. Lymphatic vessels are present throughout the parenchyma and subpleural spaces, but are absent within the alveolar capillary beds. They extend only as far as the respiratory bronchioles and alveolar ducts, leaving the gas exchange surfaces free of additional structures. However, in disease states, lymphatics can sprout in the alveolar interstitium, highlighting the need for a fine balance in disease between drainage of excess fluid, proteins, cells, etc. and ensuring adequate gas exchange can still occur.
References:
- Beatty J, Barrs V. Pleural effusion in the cat: a practical approach to determining aetiology. J Feline Med Surg. 2010;12(9):693-707.
- Fossum T. Chylothorax in Cats: Is There a Role for Surgery? J Feline Med Surg. 2001;3(2):73-79.
- Gicking JC, Aumann M. Lung lobe torsion. Compendium. 2011:E1-E6.
- Graham J, Basseches J. Liver Lobe Torsion in Pet Rabbits: Clinical Consequences, Diagnosis, and Treatment. Vet Clin North Am: Exot Anim Prac. 2014;17(2):195-202.
- Hatch A, Jandrey KE, Tenwolde MC, Kent MS. Incidence of chyloabdomen diagnosis in dogs and cats and corresponding clinical signs, clinicopathologic test results, and outcomes: 53 cases (1984-2014). J Am Vet Med Assoc. 2018;253(7):886-892.
- Hinrichs U, Puhl S, Rutteman GR. Lymphangiosarcomas in Cats: A Retrospective Study of 12 Cases. Vet Pathol. 1999.
- Ibrahim A, El-Ghareeb WR, Aljazzar A, Al-Hizab FA, Porter BF. Hepatic lobe torsion in 3 dromedary camels. J VET Diagn Invest. 2021;33(1):136-139.
- Monnet E. Lungs. In: Vol. 2, Veterinary Surgery Small Animal. Tobias K & Johnston S, ed. 1st ed. St Louis, MO: Elsevier Mosby; 2012:1762-1763.
- Mosier DA. Vascular disorders and thrombosis. In: Pathologic Basis of Veterinary Disease. Elsevier Mosby 2022:98-100.
- Radlinsky MG. Thoracic cavity. In: Vol. 2, Veterinary Surgery Small Animal. Tobias K & Johnston S, ed. 1st ed. St Louis, MO: Elsevier Mosby; 2012:1787-1812.
- Suresh K, Shimoda LA. Lung Circulation. Compr Physiol. 2016;6(2):897-943.
- Tindale C, Cinti F, Cantatore M, et al. Clinical characteristics and long-term outcome of lung lobe torsions in cats: a review of 10 cases (2000-2021). J Feline Med Surg. 2022;24(10):1072-1080.
- Valenciano AC, Arndt TP, Rizzi TE. Effusions: Abdominal, Thoracic and Pericardial. In: Cowell and Tyler's Diagnostic Cytology and Hematology of the Dog and Cat. Elsevier Mosby; 2014:259-260.
- Jubb, Kennedy, and Palmer's Pathology of Domestic Animals. Maxie MG, ed. 6th ed. St Louis, MO: Elsevier; 2016.