CASE II: H17-0922-03 (JPC 4122528).
Signalment: 4 year-old neutered male rabbit (Oryctolagus cuniculus).
History: The owner had noticed dysorexia and weight loss. A mandibular mass associated with malocclusion was diagnosed by the attending veterinarian. CT scan showed left mandibular neoplastic infiltration with osteolysis and periosteal reaction but no infiltration of the mandibular lymph nodes.
The animal was referred to the Centre Hospitalier Universitaire Vétérinaire d?Alfort (ChuvA) for a surgical exeresis with a left hemimandibulectomy. The animal died of cardiac arrest 30 minutes after the surgery during the recovery phase.
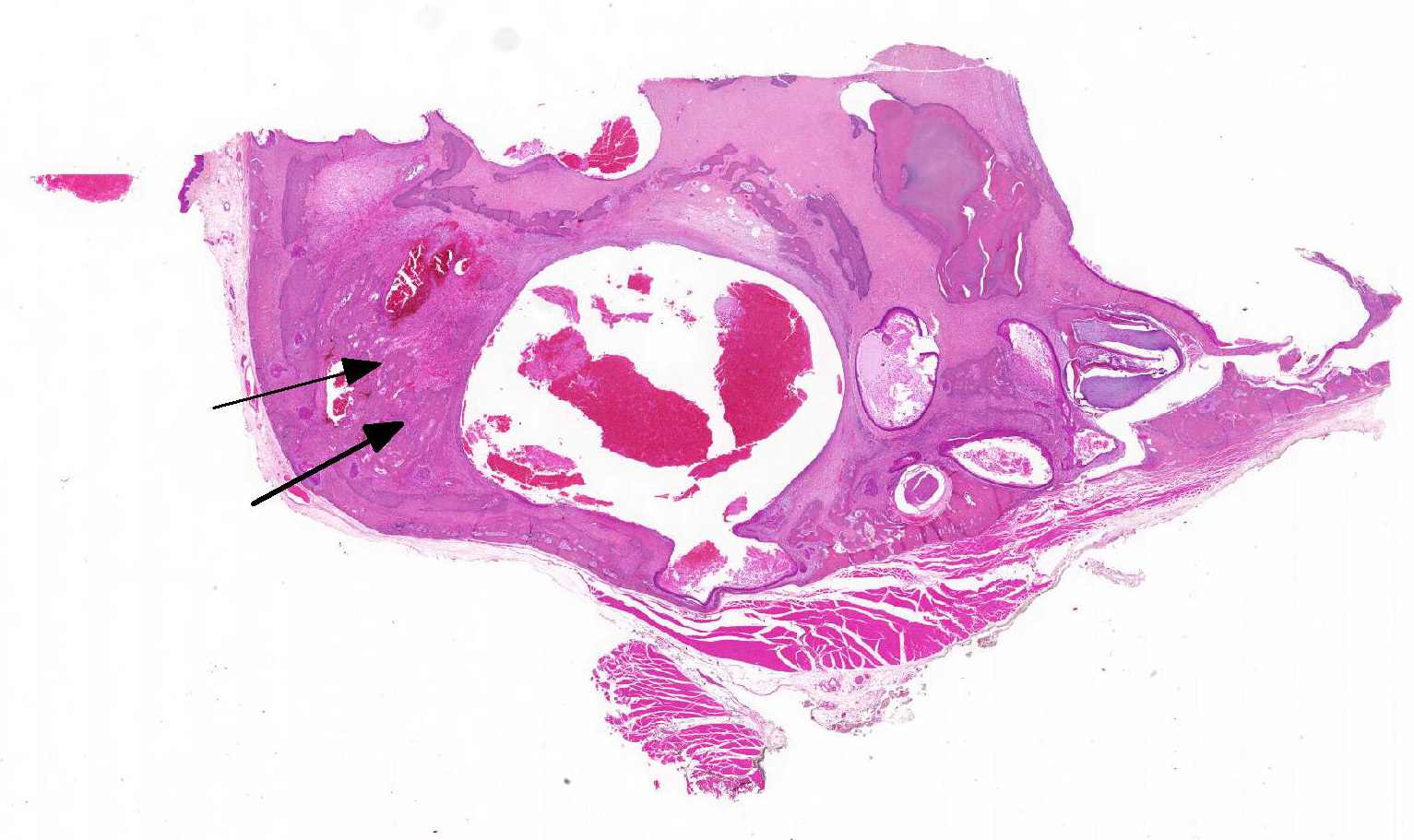
Gross Pathology: A non-ulcerated, firm, infiltrating, left mandibular mass measuring 1.5 x 2 cm in diameter with a central depressible zone caused an incisor malocclusion.
Laboratory results: NA.
Microscopic Description: Gingiva with mandibular bone:
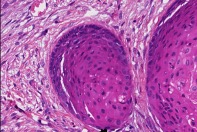
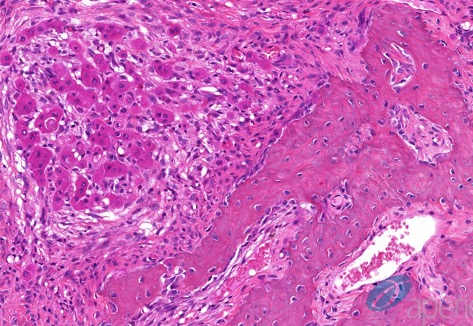
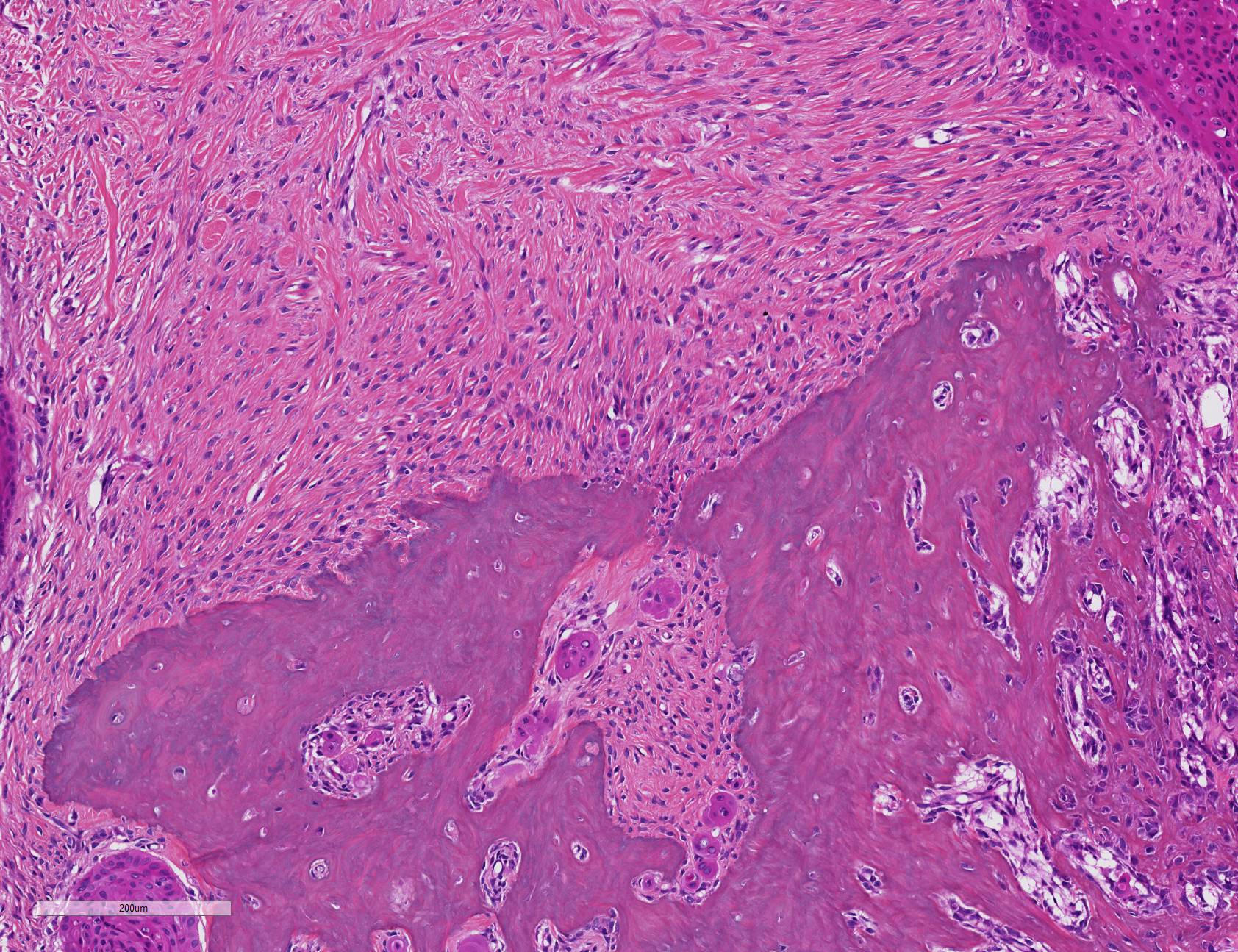
A relatively well-delineated, unencapsulated neoplasm focally infiltrates the mandibular bone. It is admixed with preexisting dental and osseous structures, and is composed of several tissue types. The first is a dense proliferative fibrous mesenchymal tissue composed of fusiform to stellate cells (reminiscent of periodontal ligament) with multifocal osseous metaplasia. The second consists in squamous epithelial nests, sometimes with cystic degeneration (accumulating desquamated cells and red blood cells in the lumen). The third component is an inconstant association of epithelial and mesenchymal structures variably mimicking normal teeth. The best differentiated areas are organized around a loose mesenchyme reminiscent of the dental pulp (ectomesenchyme), covered by a single layer of cubic to columnar cells (odontoblasts) producing an orange tubular matrix (dentin). A hypereosinophilic amorphous material (enamel) lies against the dentin; it is synthetized by a well-differentiated columnar single-layered epithelium with an inverted polarity (apical nuclei and clear basal pole) and forming palisades (ameloblasts). Their apical pole is inconstantly in contact with stellate vacuolated epithelial cells (less differentiated: stellate reticulum). The infiltrated mandibular bone in contact with the tumor is multifocally osteolytic with Howship?s lacunae containing osteoclasts and woven bone lined by osteoblasts.
Contributor Morphologic Diagnosis:
Gingiva with mandibular bone: Odontogenic tumor ? Complex odontoma
Contributor Comment: Odontogenic tumors are predominantly described in dogs and cats, and are rare in other species.3,7 Due to their similarities and the complex organization of the teeth, they present a diagnostic challenge. Identification and classification of odontogenic tumors are based on recognizing developing or fully developed teeth tissues or odontogenic epithelium.
Knowledge of odontogenesis and components of teeth is therefore essential.
Teeth develop from two embryonic tissues8:
oral cavity Malpighian epithelium and embryonic mesenchyme (ectomesenchyme). At
first, a fragment of oral Malpighian epithelium invaginates in embryonic
mesenchyme to form the dental lamina. The latter progressively differentiates
in enamel organ, an epithelial structure composed by central stellate
reticulum, lined by external and internal ameloblastic epithelium (bell stage).
The embryonic mesenchyme condenses under the internal ameloblastic epithelium
to form the ?dermal papilla?, the future dental pulp. These epithelial and
mesenchymal dental structures have an inductive effect on each other. It is
called reciprocal odontogenic induction:
1) Internal ameloblastic epithelium promotes the differentiation of the superior part of the dental papilla in an odontoblast layer.
2) Odontoblasts secrete dentin which accumulates at the odontoblasts-ameloblasts interface.
3) Presence of dentin is necessary to enamel synthesis by ameloblasts. Enamel accumulates between the dentin layer and ameloblasts.
After odontogenesis, amelobasts degenerate during dental eruption, except in hypsodont species with continuously erupting teeth (such as rodents and rabbits).
The classification and diagnosis of odontogenic tumors is based on the quantity and localization of odontogenic epithelium, production of enamel, and presence or absence of ectomesenchyme (dentin, cementum, mesenchyme resembling the periodontal ligament or the dental pulp). Visualization of dental hard tissue such as enamel, dentin or cementum is helpful in recognizing an odontogenic tumor but is an inconstant finding.3
These tumors are separated in three groups:
1) Tumors with only odontogenic epithelium (without odontogenic ectomesenchyme):
Ameloblastoma, Canine acanthomatous ameloblastoma, Ameloblastic carcinoma, Amyloid producing odontogenic tumor
2) Tumors with mesenchyme and/or odontogenic ectomesenchyme: Cementoma/cementoblastoma, Odontogenic myxoma/myxosarcoma, Peripheral odontogenic fibroma (previously called epulis)
3) Tumors with odontogenic epithelium and odontogenic ectomesenchyme (with or without hard tissue):
Ameloblastic fibroma, Infiltrative inductive ameloblastic fibroma, Ameloblastic fibro-odontoma, ameloblastic Fibro-dentinoma, Ameloblastic fibro-odontosarcoma, Complex odontoma, Compound odontoma.
In our case, the concurrent identification of dentin, odontoblasts, mesenchyme tissue resembling periodontal or dental pulp (= ectomesenchyme), as well as ameloblasts producing enamel and stellate reticulum (= odontogenic epithelium), confirms this neoplasm as an odontogenic tumor and directs the diagnosis towards a mixed odontogenic tumor. An odontoma is a dental tumor in which cell differentiation has resulted in formation of dentin and enamel. They are two types: Complex (poorly differentiated) and Compound (well differentiated, with denticle formation) 4 . The apparent disorganization of the odontogenic elements (absence of well-differentiated denticles) leads us to conclude that this particular neoplasm is a complex odontoma.
Complex odontoma are described in horses, dogs, cattle, rats and are located on the mandibular or maxillary arch. The etiology of odontomas is yet not known. Several hypotheses have been formulated: local trauma (and that continuously erupting teeth might be more sensitive to trauma), malocclusion (which may disrupt normal dental eruption), and infection.1,9
Furthermore, carcinogens such as methylnitrosourea may induce development of odontomas and other odontogenic tumors in rats.1,9 In the literature, odontomas are rarely described in rabbits but are well characterized in prairie dogs: this tumor is the third tumor in frequency (9.4%) in that species, after hepatocellular carcinoma (35.8%) and lymphoid tumors (14%); affected animals are between 2 and 6 years of age, both maxillary and mandibular arches are affected but animals only display symptoms in maxillary tumors (anatomic proximity with the hard palate, posterior choanae and the posterior nasal meatus).5
Distinguishing complex odontoma from ameloblastic fibro-odontoma can be quite challenging. In both cases, diagnosis is based on identifying odontogenic epithelium reminiscent of the enamel organ, a loose odontogenic ectomesenchyme resembling dental pulp, and several types of hard dental tissue (dentin, cementum, enamel). In some case, the diagnostis is not possible by histopathology alone.3 The age of animal and the type of tooth growth (continuously erupting or not) may be required to refine the diagnosis.
All odontogenic tumors are benign but locally aggressive. Only one case of malignant fibro-odontoma has been described, in a dog.6 Surgical excision is curative in most cases, but may be quite complex to perform.
Contributing Institution:
Unitée d'
Histologie, d'
Embryologie et
d'
Anatomie pathologique, Biopole
Departement des Sciences Biologiques et Pharmaceutiques
Ecole Nationale Veterinaire d'
Alfort
7 avenue du General De Gaulle
94704
Maisons Alfort Cedex
FRANCE
JPC Diagnosis: Gingiva and alveolar bone: Carcinoma with odontodysplasia.
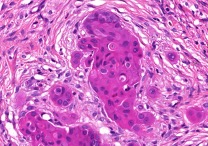
JPC Comment: In the sections we examined, the primary lesion was composed of a malignant, invasive epithelial neoplasm surrounded by a scirrhous response and woven bone proliferation. These features are consistent with a carcinoma. Potential sources for carcinoma include odontogenic epithelium (i.e. ameloblastic carcinoma; AC) or gingival epithelium (i.e. squamous cell carcinoma; SCC). There is substantial overlap between these diagnoses as both form islands of pleomorphic epithelial cells that can have some keratinization.
Generally, SCC has a greater degree of keratinization, is more inflammatory, and is associated with (potentially ulcerated) gingival mucosa. AC should have some features of odontogenic epithelium and can arise from either the gingival mucosa or deeper in submucosal connective tissue or jaw, without any evident connection to the gingival mucosa.4 In this case, although both odontogenic epithelial features (there was rare palisading of cells with antibasilar nuclei) and keratinization were present, neither were prominent. Additionally, gingival mucosa was not present in the examined sections and we could not determine if this neoplasm arose from the overlying mucosa. Taken together, we favored a more general diagnosis of ?carcinoma with odontodysplasia.?
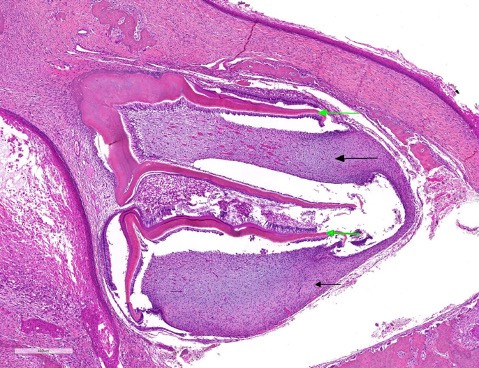
Odontodysplasia (OD) was evident in the developing teeth at the edge of the sections examined. Histologically, OD is a malformation of a tooth (or multiple teeth) or the components of a tooth. It occurs due to trauma to the dental germ during odontogenesis. Dysplastic teeth often fail to erupt.4 There is substantial histologic overlap between OD and odontoma and distinguishing between these two can be difficult to impossible. The presence of concurrent inflammation/trauma (trauma in this case was from carcinoma with abundant scirrhous response and bony proliferation) should assist the pathologist in diagnosing OD over odontoma.
(A note of thanks to Dr. Brian Murphy of UCDavis for
assistance with this very challenging case. His recent volume in oral and
maxillofacial pathology was used in the determination of the JPC morphologic
diagnosis in all of the cases this week.)
References:
1. Jang DD, Kim CK, Ahn B, Kang JS, Nam KT, Kim DJ, Han DU, Jung K, Chung HK, Ha SK, Choi C, Cho WS, Kim J, Chae C. Spontaneous complex odontoma in a Sprague-Dawley rat. J Vet Med 2002, 64 (3): 289-291.
2. Miwa Y, Nakata M, Takimoto H, Chambers JK, Uchia K. Spontaneous oral tumors in 18 rabbits (2005-2015). J Small Anim Pract 2019, https://doi.org/10.1111/jsap.13082
3. Munday JS. Lohr CV, Kiupel M. Tumors of the alimentary tract. In: Meuten DJ, ed., Tumors in Domestic Animals, 5th Ed, Ames IA: Wiley and Sons, 2017: 536-537.
4. Murphy BG, Bell CM, Soukup JW. Tumors composed of odontogenic epithelium and fibrous stroma. In: Veterinary Oral and Maxillofacial Pathology. Hoboken, NJ: Wiley and Sons, 2020: pp. 113-118
5. Pellizzone I, Vitolo GD, D?Acierno M, Stefanello D, Forlani A, Broich G. l. Lateral approach for excision of maxillary incisor pseudo-odontoma in prairie dogs (Cynomys ludovicianus). In Vivo 2016; 30: 60-68.
6. Ueki H, Sumi A, Takaishi H, Ito H, Oyamada T, Yoshikawa H. Malignant ameloblastic fibro-odontoma in a dog. Vet. Pathol 2004; 41: 183-185.
7. Uzal FA, Plattner BL, Hostetter JM. Alimentary System. In: Maxie MG ed., Jubb, Kennedy, and Palmer?s Pathology of Domestinc Animals, Vol 2.: St. Louis, MO; Elsevier, 2017.pp. 22-28.
8. https://www.askjpc.org/wsco/wsc/wsc05/05wsc04
9. https://www.askjpc.org/wsco/wsc_showcase2.php?id=YlNvSG1QSENqZ09rK0Z6d09BUmdzUT09