Conference #25
Case III:
Signalment:
Adult, female, Atlantic stingray, Hypanus sabinus
History:
This aquarium-housed Atlantic stingray initially presented to veterinary staff for a single, nodular mass on the ventral aspect of the left pectoral fin. Within one week, a second mass was noted. Excisional biopsy was elected and, at the time of surgery, multiple raised, hyperpigmented masses were found along the ventral surfaces of both pectoral fins. White purulent material was expressed from an excised nodule. Aerobic bacterial culture of the material yielded Aeromonas and Staphylococcus spp; however, no infectious agents were identified on cytology or histology. The animal was euthanized 13 months later due to a non-healing wound on the ventral pectoral girdle and progression of the nodular skin lesions along the pectoral fins.
Gross Pathology:
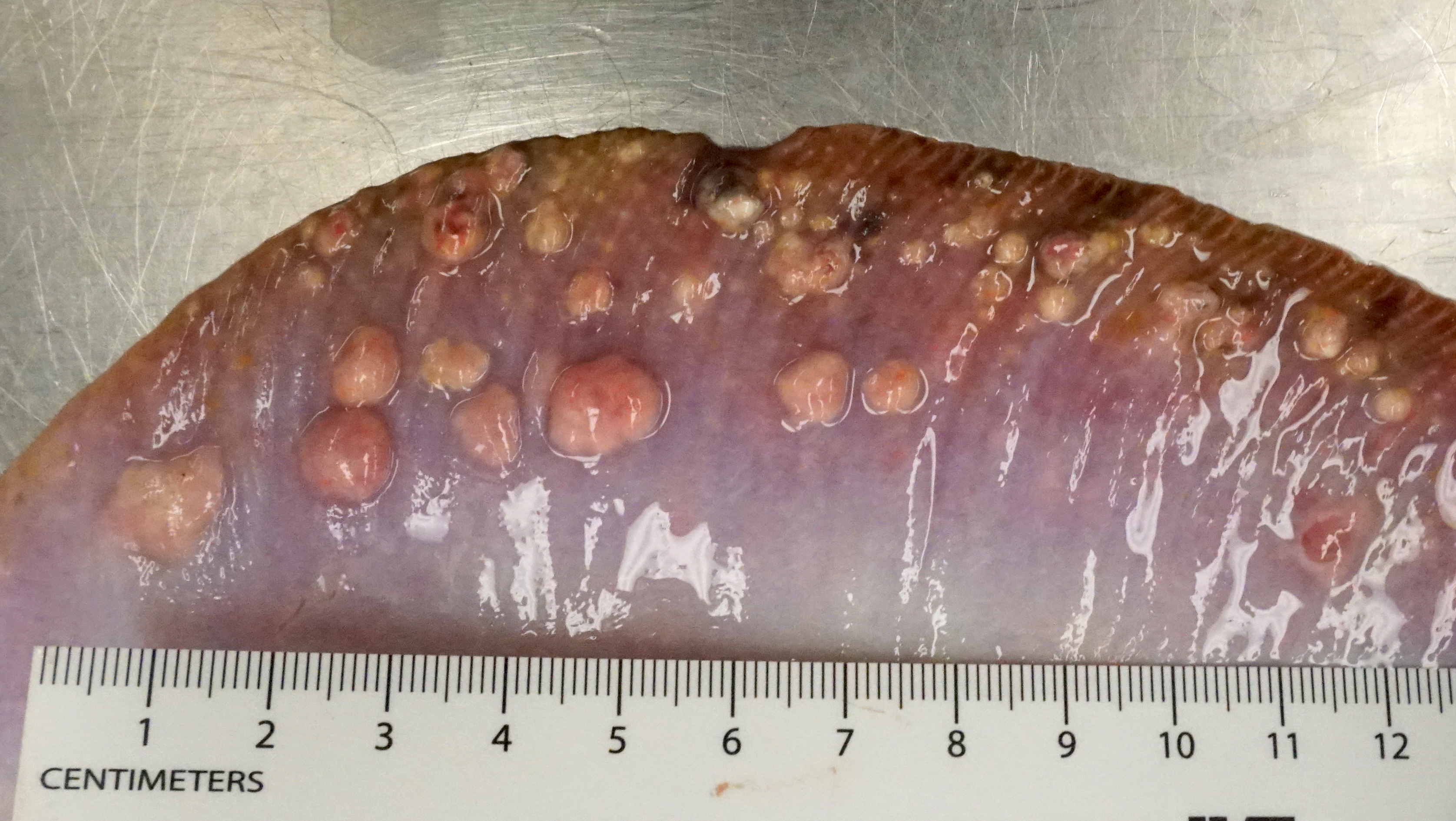
At necropsy, there were numerous (>50) firm-to-hard, well-demarcated, pale tan nodules on the ventral aspects of the pectoral and anal fins, ranging from 1-10 mm in diameter. On cut section, the nodules exuded thick, pale tan fluid. Other gross findings included a roughly 3 cm diameter cutaneous ulcer on the ventral the pectoral girdle, transudative coelomic effusion (15 ml), and multiple, 1-3 mm, firm, light tan nodules within the gill arches and along the ventral aspect of the spinal column. The liver was diffusely dark brown in color and sections sank in formalin (consistent with depleted hepatic lipid stores).
Laboratory Results:
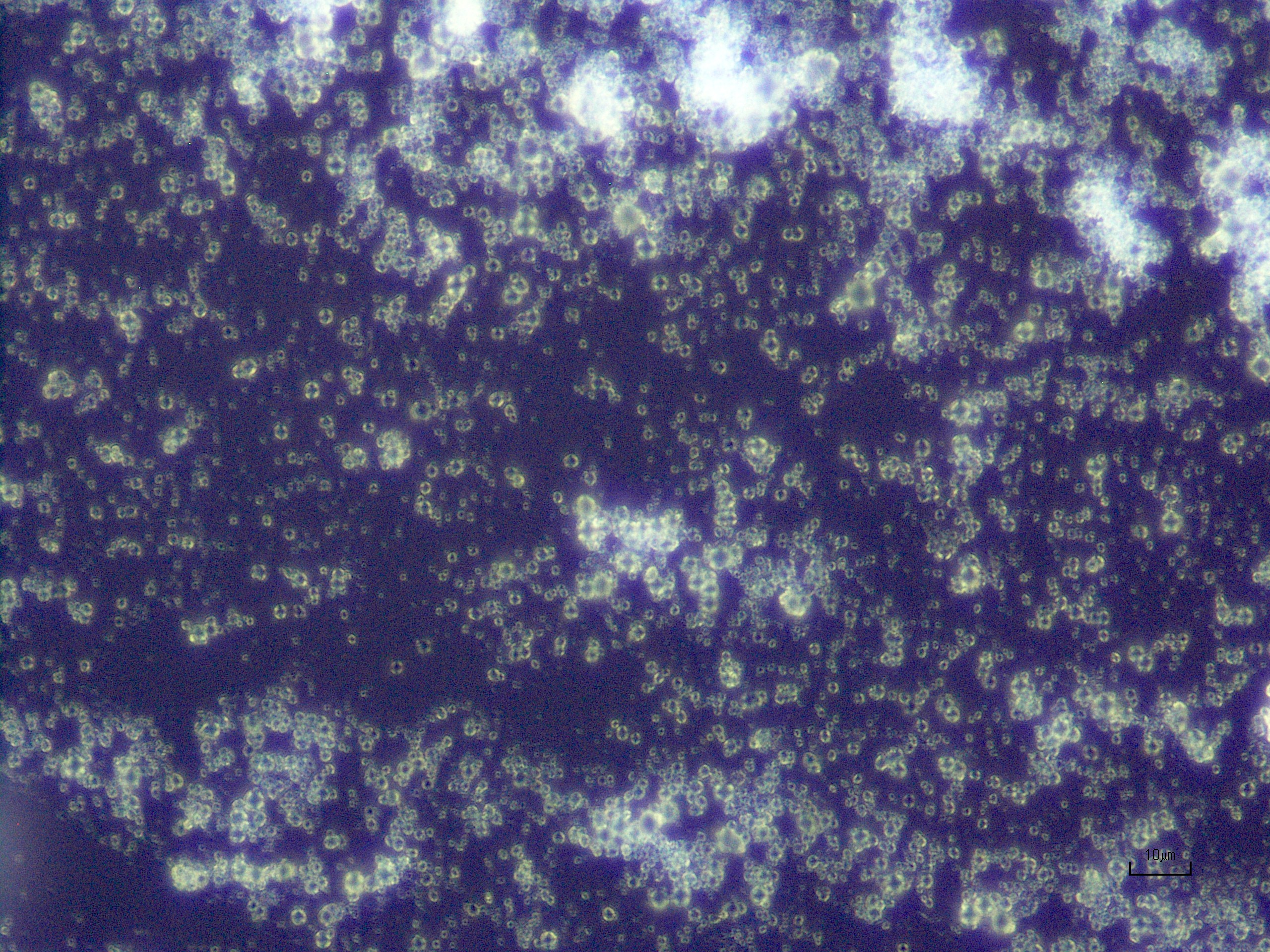
Cytology: Unstained smears of fluid collected from the skin nodules showed numerous, variably-sized, round, birefringent crystals. No infectious organisms were identified on Diff-Quik stained slides.
Microscopic Description:
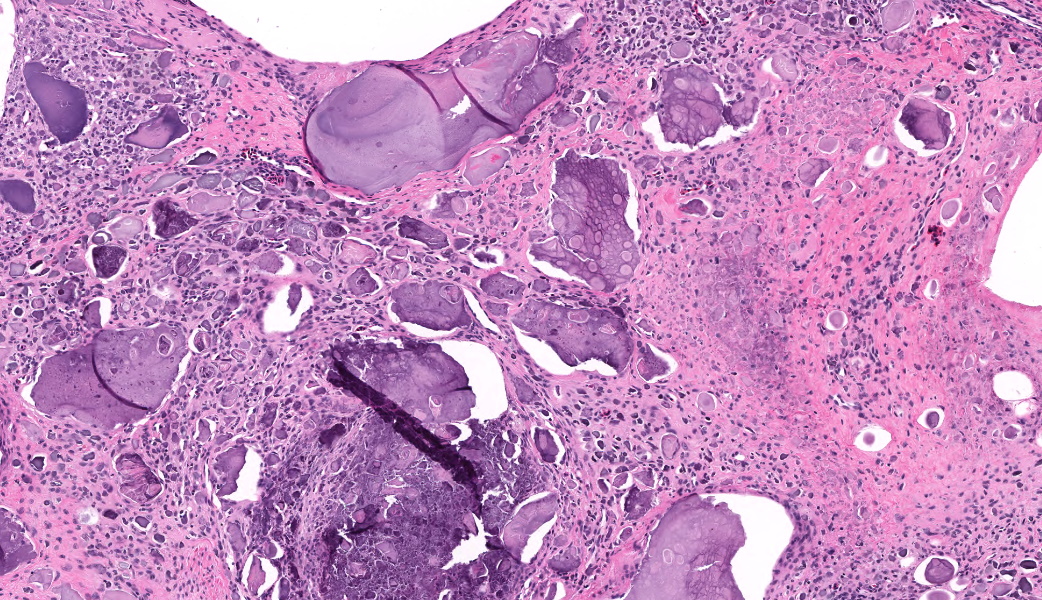
Two, full-thickness sections of pectoral fin including skin, skeletal muscle, and radial cartilage: Markedly expanding the hypodermis are multiple, variably-sized (up to 7mm diameter) nodules comprising aggregates of amorphous to finely granular, lightly to darkly-basophilic mineralized material surrounded by fibroblasts and narrow zones of dense, fibrous collagen. Both the mineralized deposits and surrounding fibrous tissue are infiltrated by variable numbers of inflammatory cells including macrophages, lymphocytes, and eosinophilic granulocytes. Occasionally, larger nodules extend into and disrupt underlying skeletal muscle and radial cartilage. There is also multifocal mineralization of the radial cartilage without associated inflammation or deformation. In the epidermis overlying the nodules there is moderate intra- and extracellular edema. Multifocal separation and loss of the epidermis may be artefactual given the lack of associated hemorrhage and inflammation.
Contributor Morphologic Diagnosis:
Skin and skeletal muscle (pectoral fin): mineralization, chronic, multifocal to coalescing, severe with fibrosis, lymphohistiocytic and granulocytic inflammation
Contributor Comment:
Gross, cytologic, and histopathologic findings in this Atlantic stingray were consistent with widespread soft tissue mineralization. In addition to the skin, nodular foci of mineralization with associated chronic inflammation and fibrosis were found within connective tissue of the gill arches and surrounding to the vertebrae. Mild, multifocal mineralization was also evident in the kidneys, liver, and choroid plexus.
Soft tissue mineralization has been reported in multiple elasmobranch species including cownose rays, a bowmouth ray, a coral catshark, and a swell shark.3,8 The diagnostic veterinary pathology service at Johns Hopkins has identified similar, but less severe, lesions in two other Atlantic stingrays from the same collection. Clinically, rays often present with firm, tan skin nodules lesions along the pectoral fins, tail, dorsal midline, and ventrum.8 The condition is progressive and can affect multiple internal organs including heart, vessels, kidneys, smooth muscle of the gills, intestines, and reproductive organs. Clinical signs include weight loss and death, likely as a result of the changes in the gills and cardiovascular system.
The pathogenesis of soft tissue mineralization in elasmobranchs is poorly understood. Gross and histomorphologic features of the nodular skin lesions closely resemble calcinosis circumscripta, which, in mammals, most commonly occurs over bony prominences and is thought to represent dystrophic mineralization related to previous trauma.5 However, involvement of internal organs in elasmobranchs is more suggestive of metastatic mineralization secondary to calcium/phosphorus imbalance. Inappropriate calcium supplementation, either in the water or diet, and underlying renal disease have been suggested as potential contributors.8 In the present case, there were histologic changes indicative of chronic kidney disease including tubular atrophy and loss, glomerulosclerosis, and interstitial fibrosis.
Though skeletal anatomy and function vary greatly among elasmobranch species, the endoskeleton generally consists of chondrocytes within an uncalcified extracellular matrix, surrounded by a fibrous perichondrium. Within the axial and appendicular skeleton, mineralized units (called "tesserae") form between the cartilage center and the outer perichondrium.1,2 In this stingray, the areas of mineralization within the cartilaginous radials of the pectoral fin (without associated deformation or inflammation) may be a variation of expected mineralization for the species.
Contributing Institution:
Johns Hopkins University, School of Medicine Department of Molecular and Comparative Pathobiology Broadway Research Building, #811 733 N. Broadway Baltimore, MD 21205 Phone: 443-287-2953 Fax: 443-287-5628 http://mcp.bs.jhmi.edu/
JPC Morphologic Diagnosis:
Fin, hypodermis and joint space: Mineralization, chronic, multifocal to coalescing, marked, with granulomatous inflammation.
JPC Comment:
This case took participants into the world of elasmobranch pathology. Dr. Holder emphasized that the primary process in this lesion was mineralization; not dermatitis, inflammation, or infection - just good, old-fashioned calcium being in places where calcium should not be.
Participants noted mineral deposition not only in the soft tissues, but also within joint spaces. Rays normally possess mineralized skeletal elements called tesserae, which may extend to articular surfaces, but the intra-articular mineral in this case was prominent enough to catch the eyes of participants. However, as mentioned by the contributor, this could be a normal variant. The literature lacks information on what degenerative tesserae look like because elasmobranch skeletal remodeling is essentially thought to be nonexistent - just tesserae-forever.
The discussion then shifted to the relevance of the stingray's liver, which was grossly described as dark brown and sank in formalin. Elasmobranchs rely on hepatic lipid stores for buoyancy and a healthy liver should float.7 A sinking liver indicates profound negative energy balance, and underscores how sick this ray was.
Tumoral calcinosis is a well-recognized but poorly understood condition in elasmobranchs. Two major forms occur - hydroxyapatite deposition disease (HADD) and calcium pyrophosphate deposition disease (CPDD).4 HADD is extremely common in reptiles, so much so that this is almost exclusively the form they get. HADD in reptiles is often accompanied by urate deposition. Crystals are granular, rounded, and have minimal, soft birefringence, as in this case.4 HADD is also associated with osteoarthritis in humans.4 CPDD, on the other hand, is most common in mammals and birds. Crystals are rhomboid to spicular with bright blue to yellow birefringence.
As a final fun fact, Dr. Holder noted that elasmobranchs can be aged (by people who have this skill) by counting the layers of tesserae in their vertebrae.5 This sounds like a sort of elasmobranch tree ring system, but sharks have the audacity to do it in cartilage instead of wood.
References:
- Dean MN, Ekstroma L, Monsonego-Ornan E, et al. Mineral homeostasis and regulation of mineralization processes in the skeletons of sharks, rays and relative (Elasmobranchii). Seminars in Cell & Develop Biology. 2015; 46: 51-67.
- Dean MN, Summers AP. Mineralized cartilage in the skeleton of chondrichthyan fishes. Zoology. 2006; 109: 164-168.
- Garner, M. M. A retrospective study of disease in elasmobranchs. Veterinary Pathology. 2013; 50(3):377-389.
- Hegazi T. Hydroxyapatite Deposition Disease: A Comprehensive Review of Pathogenesis, Radiological Findings, and Treatment Strategies. Diagnostics (Basel). 2023;13(16):2678.
- Mauldin EA, Peters-Kennedy J. Integumentary System. In: Maxie G, ed. Jubb, Kennedy, and Palmer's Pathology of Domestic Animals. 6th ed (Vol 1). St. Louis, MO. Elsevier; 2016: 509-736
- Seidel R, Lyons K, Blumer M, et al. Ultrastructural and developmental features of the tessellated endoskeleton of elasmobranchs (sharks and rays). J Anat. 2016;229(5):681-702.
- Speers-Roesch B, Treberg JR. The unusual energy metabolism of elasmobranch fishes. Comp Biochem Physiol A Mol Integr Physiol. 2010;155(4):417-434.
- Stedman NL, Garner MM. Chondrichthyes. In: Terio, McAloose, and St. Jeger eds. Pathology of Wildlife and Zoo Animals. London, UK: Academic Press; 2018: 995-1010.