Conference 24
CASE I:
Signalment:
9 years, castrated male, domestic shorthair, Felis catus, cat
History:
The cat had a history of respiratory disease diagnosed as asthma. The respiratory disease had gotten worse for two weeks prior to death. The cat had an episode of respiratory distress the evening it was taken to an emergency clinic. When placed in the carrier to be transported to the emergency clinic, the cat become extremely agitated, distressed, and was thrashing in the carrier. The cat's thrashing in the carrier eventually stopped, and the cat was dead on arrival at the emergency clinic.
Gross Pathology:
The cat was in good body condition with mild postmortem decomposition. There were small amounts of blood in the mouth, larynx, trachea and esophagus. The cranial 1/3 of the ventral and lateral aspects of the trachea were thickened by a light tan and firm mass that was firmly attached to both the right and left lobes of the thyroid gland. The right and left lobes of the thyroid gland were enlarged. The lungs were congested, heavy and wet. The heart was enlarged and weighed 24.0 grams. The myocardium of the left ventricle and interventricular septum of the heart were diffusely thickened with a small slit-like left ventricular lumen. The myocardium of the right ventricle of the heart was variably thickened.
Laboratory Results: There was no additional testing performed.
Microscopic Description:
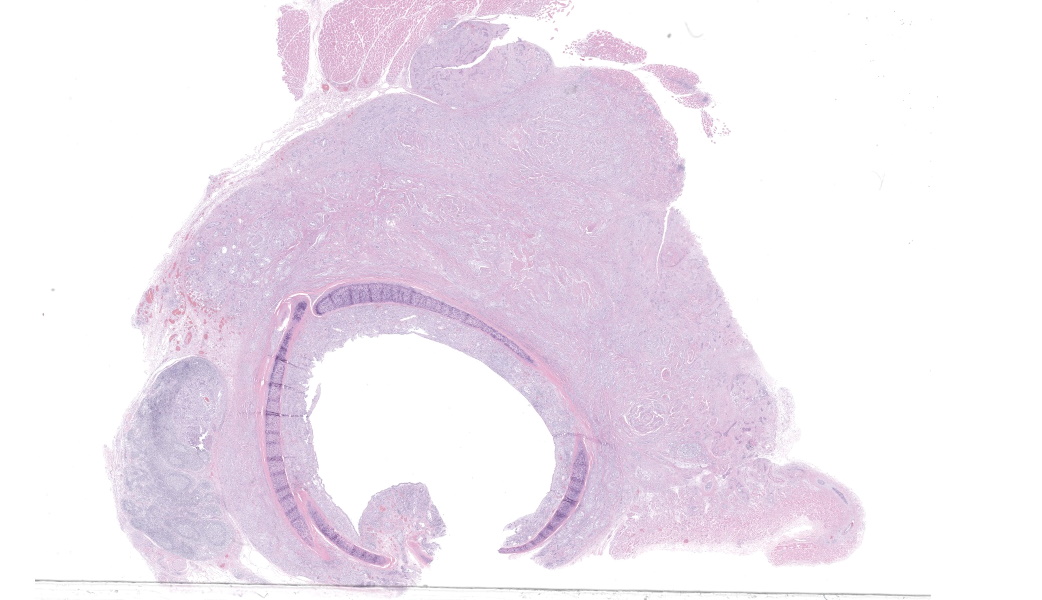
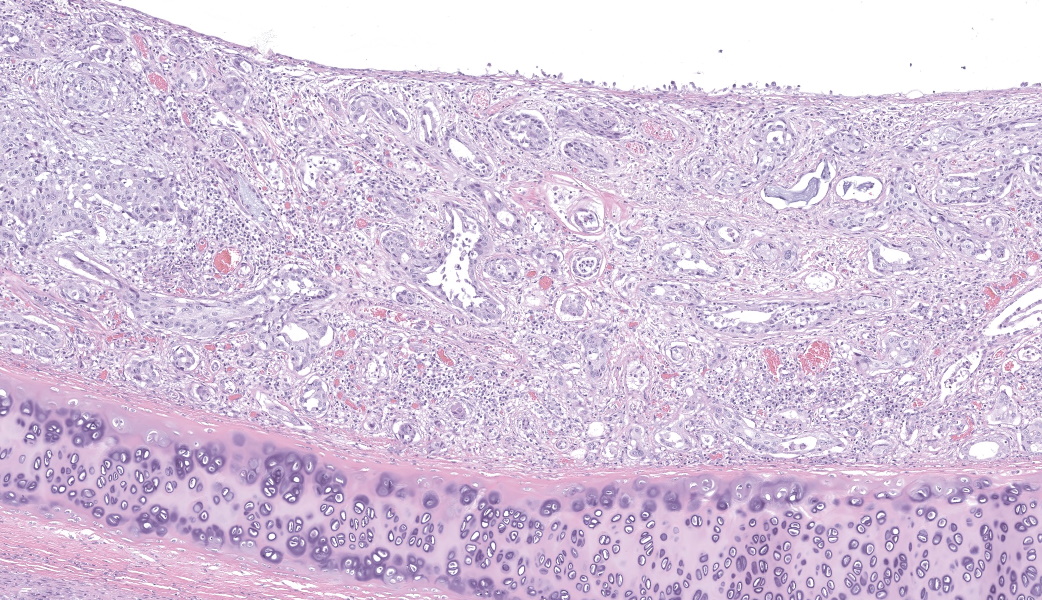
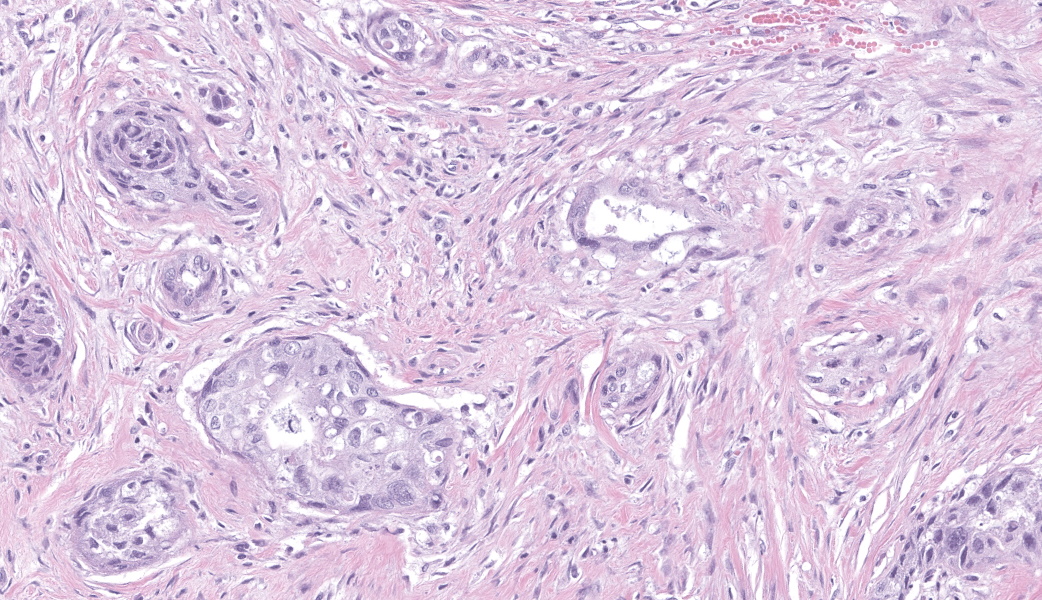
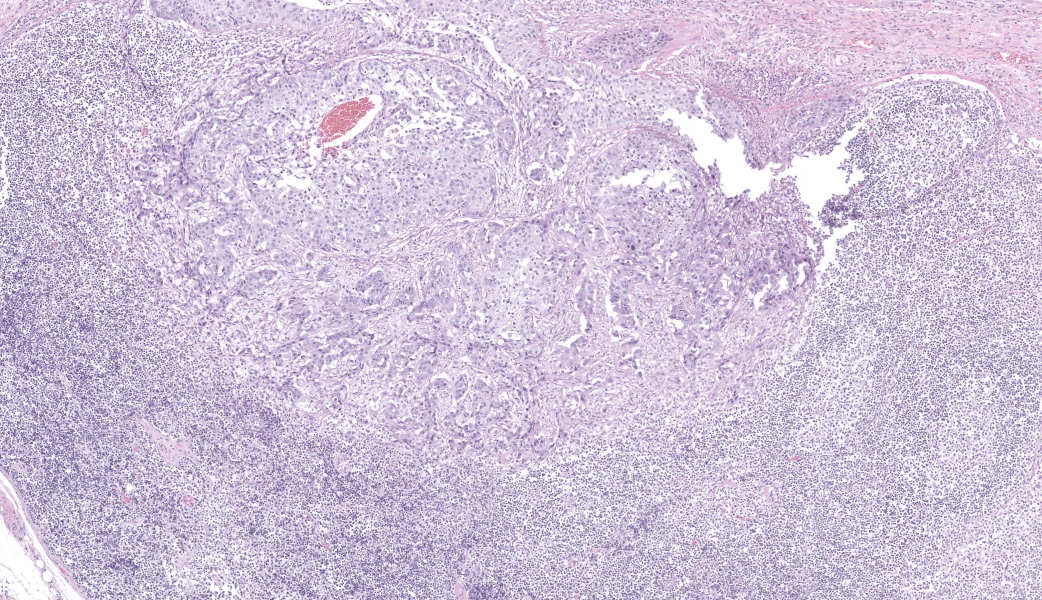
The mucosal epithelium of the grossly affected trachea is multifocally eroded to ulcerated. The eroded and ulcerated tracheal mucosa is covered by a coagulum of fibrin, cellular debris and neutrophils. Where it is intact, there is multifocal squamous metaplasia of the tracheal mucosal epithelium (not present in every slide). Clusters and trabeculae of neoplastic squamous epithelial cells suspended in a proliferative fibrovascular stroma variably thicken the submucosa deep to the intact tracheal mucosal epithelium. There are small numbers of clusters that have clear centers filled with variable amounts of cellular and necrotic debris resembling tubules. The neoplastic cells are round to polygonal with distinct cell borders, lightly eosinophilic cytoplasm and a large round nucleus. There is mild cellular and nuclear pleomorphism. There are three mitotic figures per ten high power fields. There is multifocal necrosis of the tracheal cartilage rings (not present in every slide). The peritracheal fat and skeletal muscle contain a large invasive mass of neoplastic squamous epithelial cells that encircle the right and left vagus nerves (not present in every slide). The neoplastic cells are arranged in clusters and trabeculae suspended in a dense and proliferative fibrovascular stroma. There are foci of necrosis in the mass. The cervical lymph nodes in the area contain neoplastic cells (not present in every slide).
Contributor Morphologic Diagnosis:
Trachea: Nonkeratinizing squamous cell carcinoma
Contributor Comment:
Neoplasia of the trachea in cats is rare with most reports of neoplasia in the upper respiratory tract being in the larynx rather than the trachea.2,3,4,5,6,8 The most commonly reported tracheal neoplasms in cats are lymphoma and carcinomas.2,4 The reported tracheal carcinomas in cats include adenocarcinoma, squamous cell carcinoma, seromucinous carcinoma, tracheobronchial neuroendocrine carcinoma and carcinoma.2,4 Squamous cell carcinomas were the most common tracheal carcinoma in one study of tracheal neoplasia in cats, but lymphoma was the most common tracheal neoplasia.4 Tracheal neoplasia tends to occur in middle age to older cats with median ages reported as 9 years and 12 years of age.2,4 In one study, more female cats had tracheal neoplasia than male cats.4 In the same study, Siamese cats were predisposed to develop tracheal lymphoma. Domestic longhair cats were predisposed to develop tracheal lymphoma and adenocarcinoma. However, there are so few cats with reported tracheal neoplasia that these findings may not be accurate.
Cats with tracheal neoplasia typically have nonspecific clinical signs of airway obstruction including dyspnea, wheezing, coughing, gagging, and stridor.2,4,5,6 These clinical signs are not specific for tracheal neoplasia and are common with a variety of respiratory diseases including feline asthma, which was the initial diagnosis for the respiratory disease in this cat.5,6 Because they are rare and the clinical signs are not specific, the diagnosis of tracheal neoplasia is often not made until the disease is advanced.2,4 Thus, cats diagnosed with tracheal neoplasia often have short survival times with reported overall median survival times of 15.5 days and 121 days with therapy.4 In this case, the diagnosis of tracheal neoplasia was not made until the postmortem examination. The cat also had hypertrophic cardiomyopathy that based on the clinical history was likely to have contributed greatly to the death of the cat with the potential development of a fatal cardiac arrhythmia.
Contributing Institution:
New Mexico Department of Agriculture Veterinary Diagnostic Services
https://www.nmda.nmsu.edu/nmda-homepage/divisions/vds/JPC Morphologic Diagnosis:
Trachea: Adenosquamous carcinoma.
JPC Comment:
This year's 24th conference was moderated by Dr. Francisco Carvallo, a respiratory and infectious disease expert from the Virginia-Maryland College of Veterinary Medicine and a first-time moderator for the WSC! Following an excellent pre-conference lecture on the specifics and updated terminology of interstitial pneumonia, participants were treated to a respiratory-focused conference that opened with this surprisingly controversial case!
Diagnoses amongst participants on the precise origin of this tumor (from the mucosal epithelium or the submucosal glandular epithelium were varied due to the significant formation of tubules and acini by this neoplasm with only rare individual cell dyskeratosis. An Alcian blue stain was underwhelming due to significant background staining of tracheal mucus and ground substance, but there were some neoplastic acini that contained strongly Alcian blue-positive luminal material, indicating that neoplastic cells may be producing mucin. Additionally, the neoplastic cells lacked immunoreactivity for p63 and p40, making a diagnosis of squamous cell carcinoma less likely. Based on the morphology of the neoplasm and the suggestive results of the Alcian blue stain, the JPC decided on a diagnosis of adenosquamous carcinoma. Adenosquamous carcinoma is a rare, aggressive epithelial neoplasm that demonstrates both malignant squamous epithelial differentiation and a malignant glandular component within the same tumor.7 Adenosquamous carcinomas tend to be highly infiltrative in the organs in which they arise and carry a poor prognosis.7
This neoplasm induced an impressive desmoplastic response in the surrounding connective tissue. Dr. Carvallo reviewed the pathogenesis of desmoplasia with conference attendees, talking through tumor cell signaling leading to activation of "cancer-associated fibroblasts" (CAFs) within the tumor microenvironment. Activation of CAFs induces signal transduction of pro-growth pathways that upregulate profibrotic genes, leading to production and remodeling of the extracellular matrix (ECM).1 The increased density of the ECM can physically impede the delivery of therapeutic drugs, make it more difficult for T lymphocytes and NK cells to access the tumor (immune evasion), and enable tumor growth via sequestration of growth factors.1 Additionally CAFs promote angiogenesis and epithelial-to-mesenchymal transition (EMT) to facilitate migration, invasion, and metastasis.1
References:
- Asif PJ, Longobardi C, Hahne M, Medema JP. The Role of Cancer-Associated Fibroblasts in Cancer Invasion and Metastasis. Cancers (Basel). 2021;13(18):4720.
- Carlisle CH, Biery DN, Thrall DE. Tracheal and laryngeal tumors in the dog and cat: literature review and 13 additional patients. Vet Radiol. 1991;32(5):229-235
- Caswell JL, Williams KJ. Respiratory system. In: Maxie MG, ed. Pathology of Domestic Animals. 6th ed, vol. 2. St. Louis, MO: Elsevier; 2016:480-483
- Jakubiak MJ, Siedlecki CT, Zenger E, et al. Laryngeal, laryngotracheal, and tracheal masses in cats: 27 cases (1998-2003). J Am Anim Hosp Assoc. 2005;41:310-316
- Jelinek F, Vozkova D. Carcinoma of the trachea in a cat. J Comp Path. 2012;147:177-180
- Lobetti RG, Williams MC. Anaplastic tracheal squamous cell carcinoma in a cat. Tydskr S Afr vet Ver. 1992;63(3):132-133
- Mehrad M, Trinkaus K, Lewis JS Jr. Adenosquamous Carcinoma of the Head and Neck: A Case-Control Study with Conventional Squamous Cell Carcinoma. Head Neck Pathol. 2016;10(4):486-493.
- Wilson DW. Tumors of the respiratory tract. Meuten DJ, ed. Tumors in Domestic Animals. 5th ed. Ames, IA: Wiley Blackwell; 2017:479.