Wednesday Slide Conference 2023-2024Signalment:
14-year-old, American Paint gelding, horse (Equus caballus)
History:
The horse presented to its primary care veterinarian for an approximately 3 cm in diameter mass on the right facial crest that had been present for about two months. The mass began increasing in size two weeks prior to presentation. An in-house fine needle aspiration (FNA) cytology revealed ‘macrophages and bacteria’. On ultrasonography the mass was noted to have a soft tissue echogenicity, lobulated appearance and several small fluid-filled pockets throughout.
Gross Pathology:
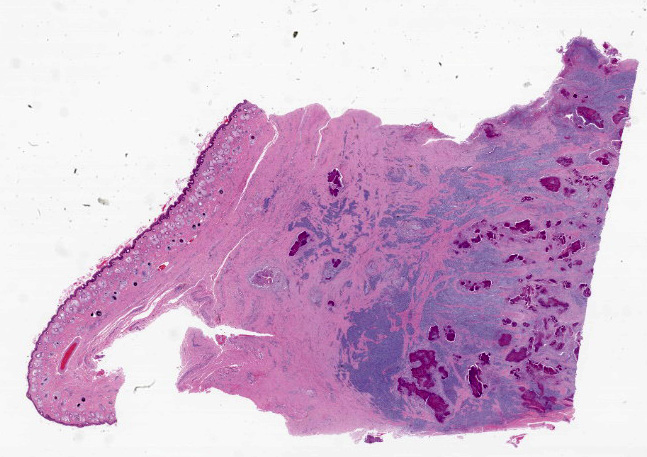
The mass was excised and submitted for histologic examination. The mass was transected prior to submission into two, approximately 5.0 x 2.0 cm, triangle-shaped sections of haired skin. On cut section there were multiple, variably sized and shaped foci that contained a yellow granular material.
Microscopic Description:
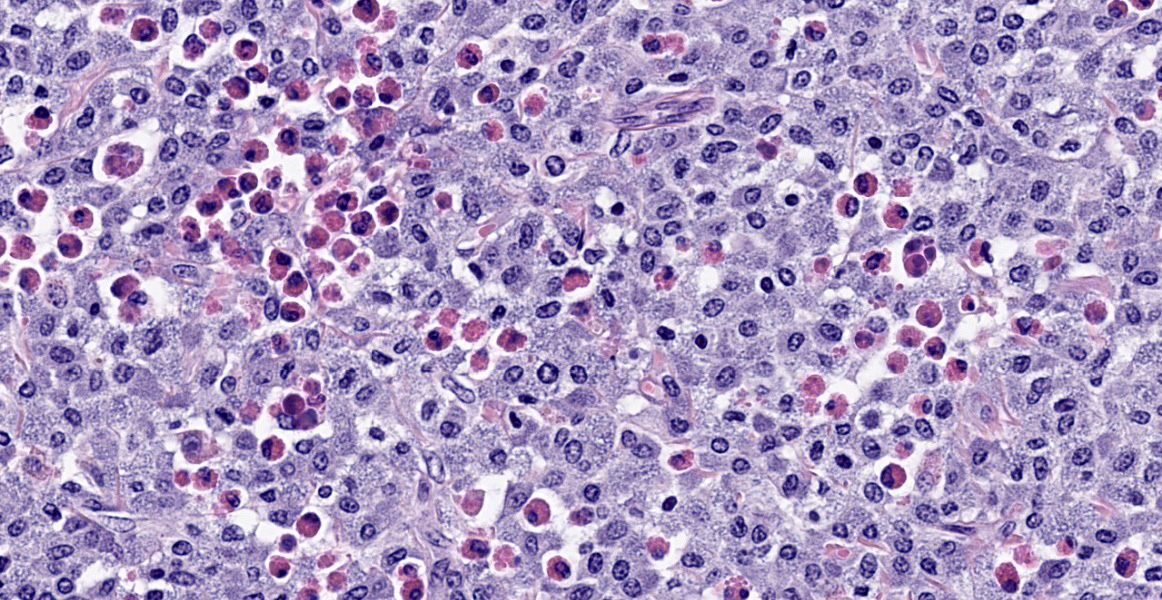
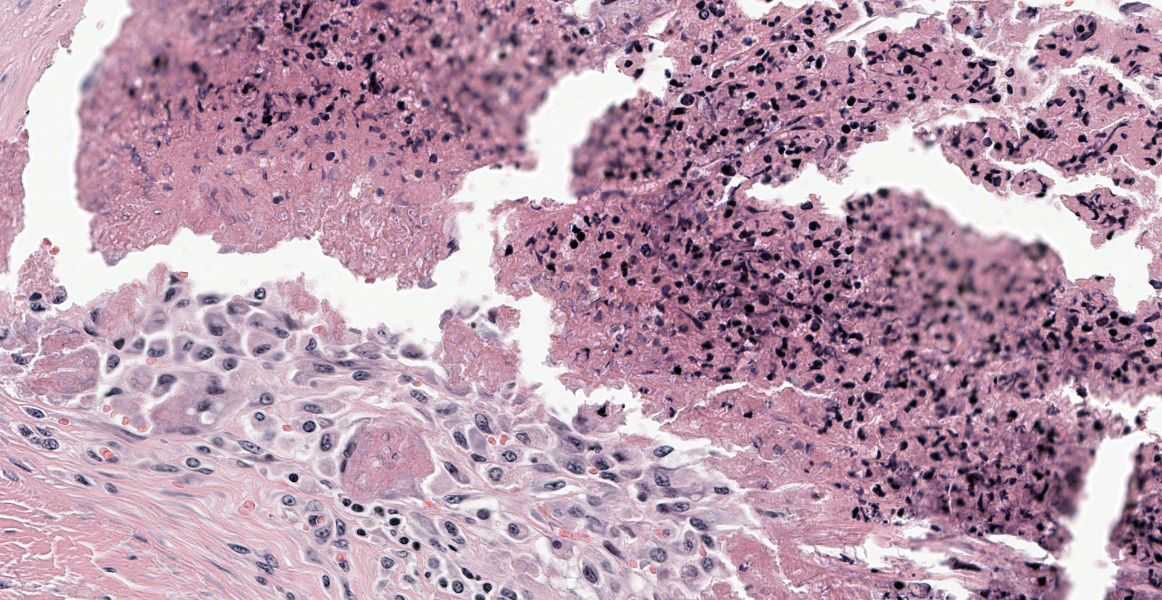
Haired skin, right facial crest: On histologic examination there is a poorly demarcated, nonencapsulated, non-compressive mass in the hypodermis. The mass extends to the lateral and deep surgical borders. The mass comprises islands and sheets of individualized round cells, supported by a dense collagenous stroma. The round cells have distinct cell borders and a moderate to high nuclear to cytoplasmic ratio. The cytoplasm is scant to moderate, grey blue and coarsely granular. The intracytoplasmic granules stained positively with toluidine blue stain (mast cell granules). The nucleus was centric, round to oval with a finely reticular chromatin pattern and a small to inconspicuous nucleolus. Mitotic figures are not present in the sections examined. Comprising approximately 30-40% of the area of the neoplasm are multiple, variably-sized (100-700µm ), irregularly shaped, bright pink foci of necrosis with a central core of disintegrating inflammatory cells (eosinophils) and karyorrhectic debris, a peripheralized layer of multinucleated giant cells, foamy macrophages and a few layers of fibroblasts. Neoplastic mast cells, admixed with moderate numbers of eosinophils and a few lymphocytes, surround these foci.
Contributor’s Morphologic Diagnosis:
Cutaneous mast cell tumor.
Contributor’s Comment:
Mast cell tumors are relatively uncommon in horses. They are usually benign tumors, with only a few reports where they show aggressive behaviour. Equine cutaneous MCTs are reported to commonly affect head, neck, trunk and limb.1,2 They are rarely reported to affect other areas such as upper respiratory tract, oral cavity and eye.2 There is a predilection in males, and no apparent breed predilection. The majority of these tumors are non-pruritic and non-painful.3 They show slow, progressive growth or become static, even over a course of two years.2 Rarely a lesion may show sudden rapid growth.1 Equine mast cell tumors are also called mastocytosis or mastocytoma due to their clinical features and benign behaviour. There is some discussion in the literature regarding their representation as a true neoplastic process.1,2,3
Histologically, they manifest as well demarcated masses in the dermis or subcutis, comprised of sheets of well-differentiated mast cells admixed with a few eosinophils and prominent areas of necrosis, fibrosis and dystrophic mineralization and rare mitotic figures.2,3 The mast cell granules are often numerous but difficult to visualize with routine hematoxylin and eosin staining.2 Histochemical stains to highlight the mast cell granules were performed in this case (toluidine blue and Luna stains) and confirm the diagnosis. Histological grading schemes do not exist for equine cutaneous MCTs. Prognosis is usually good and complete surgical excision is curative. Recurrence after surgical excision is uncommon. Spontaneous regression has been reported in cases with incomplete surgical excision.
Contributing Institution:
Department of Veterinary Pathology and Prairie Diagnostic Services
Western College of Veterinary Medicine,
University of Saskatchewan
52 Campus Drive
Saskatoon, Saskatchewan
S7N 5B4 Canada
JPC Diagnosis:
Haired skin: Mast cell tumor.
JPC Comment:
Equine mast cell tumors (MCTs) may present a diagnostic challenge when first encountered due to a few unique histologic features. As in other species, equine MCTs contain round cells with pale eosinophilic cytoplasm often separated by collagen fibers and accompanied by eosinophils. Unlike in other species, equine MCTs may contain large lakes of eosinophilic debris surrounded by fibrosis. Mast cells may be fewer than in MCTs from other species and cytoplasmic granules may be inapparent until revealed by toluidine blue or Giemsa staining. Tumors may also mineralize extensively with chronicity, leading to radiologically visible calcification.2
The development and proliferation of mast cells is regulated by stem cell factor (SCF), the ligand for the c-kit gene product KIT, a tyrosine kinase receptor also known as CD117.4 In many canine MCTs, c-kit mutations cause activation of KIT in the absence of SCF, resulting in aberrant stimulation of pro-growth signaling pathways. Studies suggest that c-kit mutations may play a substantial role in the neoplastic transformation of mast cells in dogs and that differing KIT expression patterns can be used to assess grade, prognosis, and risk of recurrence.4
KIT expression, assessed with IHC staining using anti-KIT antibodies, is classified into three patterns, denoted by the numerals I-III. KIT staining pattern I consists of a membranous staining pattern, the expected localization for a transmembrane receptor tyrosine kinase; pattern II consists of focal to stippled cytoplasmic staining; and pattern III is characterized by diffuse cytoplasmic staining.5 In well-differentiated canine MCTs, KIT expression is generally in a type I pattern, while high grade tumors have predominantly type II and III labelling; thus, translocation of KIT from the plasma membrane to the cytoplasm is associated with tumor recurrence and shorter overall survival times.5
In contrast to canine MCTs, in which grading and prognostic indices are well established, only two studies have assessed how morphologic features, proliferative activity, or KIT expression patterns can be used to predict biologic behavior in equine MCTs.1,4 These two studies reached contradictory conclusions. The first found that KIT staining patterns and histologic features were not associated with poor clinical outcome or abnormal tumor behavior.1 By contrast, the most recent study found that most equine MCTs were composed of mast cells with mild anisokaryosis, a low proliferative rate, and a dominance of KIT pattern I staining, representing well-differentiated MCTs and benign behavior.4 Approximately one-third of cases in this study were comprised of mast cells exhibiting more infiltrative growth, moderate to marked anisokaryosis, a higher degree of proliferation, and KIT staining patterns II and III, representing poorly-differentiated MCTs associated with more potentially aggressive behavior.4 These results indicate that it may be possible, as in canine MCTs, to make hay out of differential KIT staining to identify the small subset of potentially more aggressive equine MCTs. More research is needed to define the associations among biological behavior, morphology, proliferative indices, and KIT expression patterns in equine MCTs.4
This week’s moderator, JPC’s very own Dr. Bruce Williams, discussed this entity as one in which diagnosis is typically made on H&E evaluation alone. Toluidine blue and Giemsa stains can be used to visualize initially inapparent mast cell granules, and equine MCTs do show expected positive immunoreactivity to CD25, CD117, and tryptase, but the unique histologic appearance of equine MCTs usually obviates the need to pony up the time and money for histochemical and immunohistochemical stains.
The primary differential diagnosis for equine MCTs is equine collagenolytic granulomas, which contain, as the name implies, large numbers of eosinophils; however, collagenolytic granulomas often contain flame figures and do not contain the lakes of eosinophilic debris and sheets of mast cells characteristic of equine MCTs.
References:
- Clarke L, Simon A, Ehrhart EJ, et al. Histologic characteristics and KIT staining patterns of equine cutaneous mast cell tumors. Vet Pathol. 2014;51(3):560-562.
- Mair TS, Krudewig C. Mast cell tumors (mastocytosis) in the horse: a review of the literature and report of 11 cases. Equine Vet Educ. 2008;20(4):177-182.
- Millward LM, Hamberg A, Mathews J, et al. Multicentric mast cell tumors in a horse. Vet Clin Pathol. 2010;39(3):365?370.
- Ressel L, Ward S, Kipar A. Equine cutaneous mast cell tumours exhibit variable differentiation, proliferation activity and KIT expression. J Comp Pathol. 2015;153(4):236-243.
- Webster JD, Yuzbasiyan-Gurkan V, Kaneene JB, Miller RA, Resau JH, Kiupel M. The role of c-KIT in tumorigenesis: evaluation in canine cutaneous mast cell tumors. Neoplasia. 2006;8(2):104-111.