Signalment:
Gross Description:
Histopathologic Description:
Morphologic Diagnosis:
Lab Results:
Condition:
Contributor Comment:
The cause of pulmonary hyalinosis is unknown. Some pathologists consider it an incidental finding in older dogs (3), while others postulate that it is a response to inhalation of dust or pneumotoxicants such as silica in uranium ore dust (1) or to non-specific aspirated material (2). This dog did not have any evidence of aspiration and it is unknown whether the unusual material in the lung was also present in the enclosure or environmental surroundings.Â
Unfortunately, the definitive cause of death in this dog remained inconclusive. The most significant findings were changes found in the lungs and kidneys and the overall poor body condition. The pulmonary lesions involved only a relatively small portion of the overall volume of lung (about 10%), however where the lesions were present, the normal architecture was completely obliterated. Additionally a moderate, chronic, multifocal-segmental, membranoproliferative glomerulonephritis was detected microscopically. Although no biochemical testing of renal function and urinalysis were done in this dog, there was no evidence of uremic lesions at necropsy, which could have indicated uremia or renal failure. However, as glomerular disease can cause protein loss, this lesion could have potentially contributed to the poor body condition of this dog.Â
Although the dog was thin at the time of death, it was not emaciated, as visceral and marrow fat stores were still present, and there was no histologic evidence of hepatocyte or pancreatic atrophy. Abundant food stuffs were present in the stomach, however the long-term food consumption and therefore energy intake of this dog was unknown. Increased food energy is required in animals living in a cold environment to maintain adequate body temperature, so inadequate food intake would also have to be considered as a possible contributing factor to this dog being very thin.Â
JPC Diagnosis:
Conference Comment:
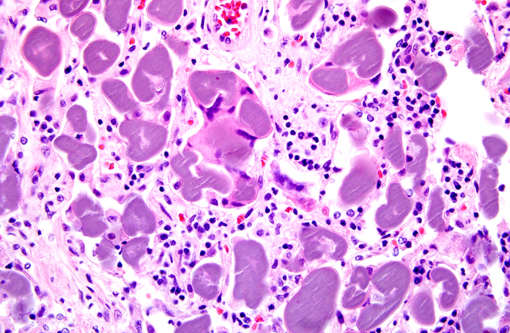
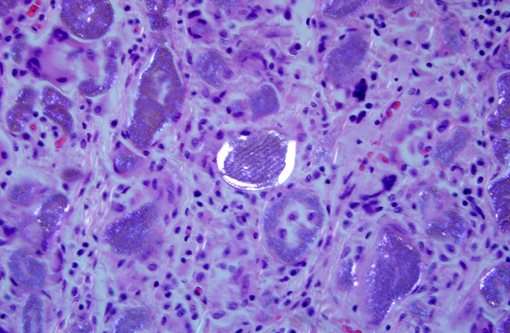
In 1972, Dr. Leonard Billups of the Armed Forces Institute of Pathology reported that the canine condition now known as pulmonary hyalinosis was not composed of plant material as in pulse pneumonias; the hyaline bodies in dogs ( known colloquially as Billups bodies) did not stain with silver impregnation stains as leguminous cotyledons do (2).Â
Pulmonary hyalinosis may be differentiated from other conditions based upon histologic and staining features. The hyaline bodies are intracellular in macrophages and multinucleated giant cells, occasionally calcify, are birefringent, positive for periodic acid-Schiff (PAS), crystal violet and oil red 0, and ultrastructurally consist of a whorled arrangement of lamellar membranes suggestive of degenerate cells (1,5). Corpora amylacea are rounded, basophilic hyaline masses that are often concentrically laminated. Corpora amylacea are not birefringent, do not calcify, and are weakly PAS positive. Pulmonary microliths are often distributed throughout the lung, and the calcospherites that compose this lesion are concentrically laminated, have radial striations, are calcified, and are intensely positive with PAS and colloidal iron stains, and unlike pulmonary hyalinosis, the material is extracellular (6).Â
References:
2. Billups LH, Liu SK, Kelley DF, Garner FM. Pulmonary Granulomas Associated with PAS-Positive Bodies in Brachycephalic Dogs. Vet Pathol 1972; 9: 294-300.Â
3. Caswell JL, Williams KJ. Respiratory system. In: Maxie MG, ed. Jubb, Kennedy and Palmers Pathology of Domestic Animals. Vol. 2, 5th ed. Philadelphia, PA: Elsevier-Saunders; 2007: 572-573.Â
4. Knoblich R. Pulmonary granulomatosis caused by vegetable particles: socalled lentil pulse pneumonia. Am Rev Respir Dis. 1969;99:380389.Â
5. Harrison JD, Martin IC. Oral vegetable granuloma: ultrastructural and histological study. J Oral Pathol. 1986;15:322326.Â
6. Rhee DD, Wu ML. Pulse Granulomas Detected in Gallbladder, Fallopian Tube, and Skin. Arch Pathol Lab Med. 2006;130:18391842.Â