Conference 23
CASE I:
Signalment:
2-year-old, neutered male, German shepherd dog, Canis lupus familiaris, canine
History:
This dog presented to the referring veterinarian for a three-month history of lethargy and neurologic signs, including a hypermetric gait and ataxia. Spinal radiographs and bloodwork were within normal limits. Given prior medical history of testing positive for Lyme borreliosis and anaplasmosis, doxycycline was prescribed, and the dog was referred to a neurologist. Neurological examination revealed hypermetria of the right forelimb, combined vestibular and sensory ataxia, and a broad-based stance. There were "slightly increased cells" in the cerebrospinal fluid and an MRI of the brain was within normal limits. The dog was treated with clindamycin and prednisone for suspected encephalitis. Three weeks later, a urine sample was negative for Blastomyces dermatitidis antigen, and a cervical MRI was within normal limits; treatment with doxycycline, clindamycin, and prednisone was continued. One month following the initial presentation, the dog's energy level and appetite had improved, but the dog continued to exhibit mild hypermetria in all four limbs. A recheck cerebrospinal fluid tap was within normal limits. Antemortem diagnostics for infectious diseases including Toxoplasma gondii, Neospora caninum, Cryptococcus neoformans, and Blastomyces dermatitidis all yielded negative results. Nerve and muscle biopsies were performed, and the nerve biopsies indicated possible increased fat droplets with a "possible suggestion of carnitine deficiency." The dog was started on gabapentin and enrofloxacin and was continued on prednisone and clindamycin. The dog continued to decline despite treatment, and was euthanized approximately three months after the initial presentation and submitted for necropsy.
Gross Pathology:
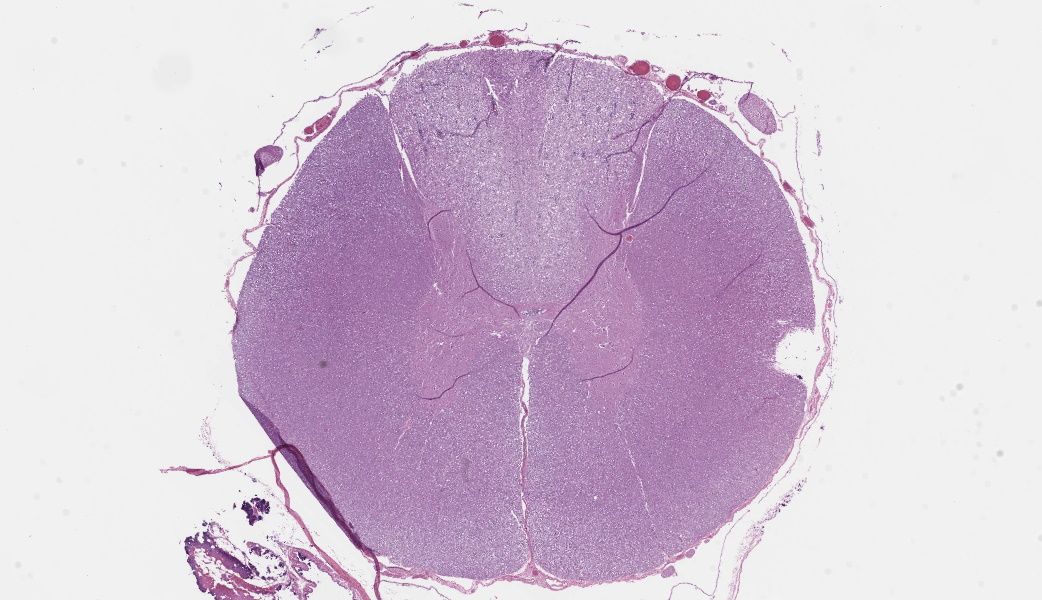
After fixation and trimming, the cross sections of the entire length of the spinal cord exhibited well-demarcated, wedge or V-shaped, off-white pallor of the dorsal funiculi.
Laboratory Results: None.
Immunohistochemistry (IHC):
The following IHC preparations were performed:
Spinal cord:
Canine distemper virus antigen: There was no immunoreactivity (negative).
Borrelia burgdorferi antigen: The results were equivocal with mild non-specific immunoreactivity.
Brain:
Canine distemper virus antigen: There was no immunoreactivity (negative).
Canine herpesvirus antigen: There was no immunoreactivity (negative).
Canine adenovirus (CAV-1 and CAV-2) antigen: There was very little immunoreactivity (equivocal result).
Microscopic Description:
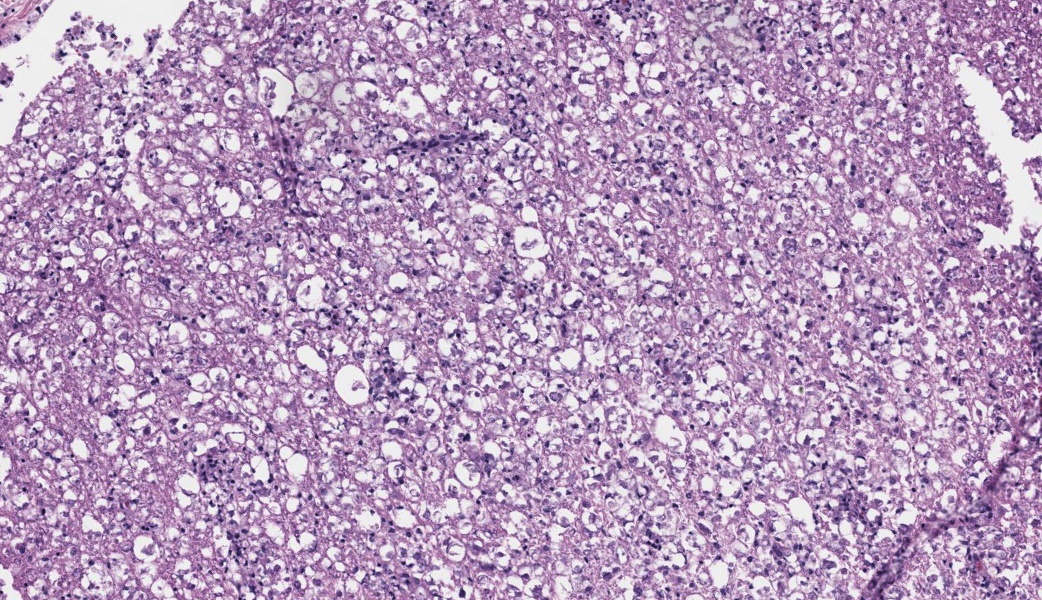
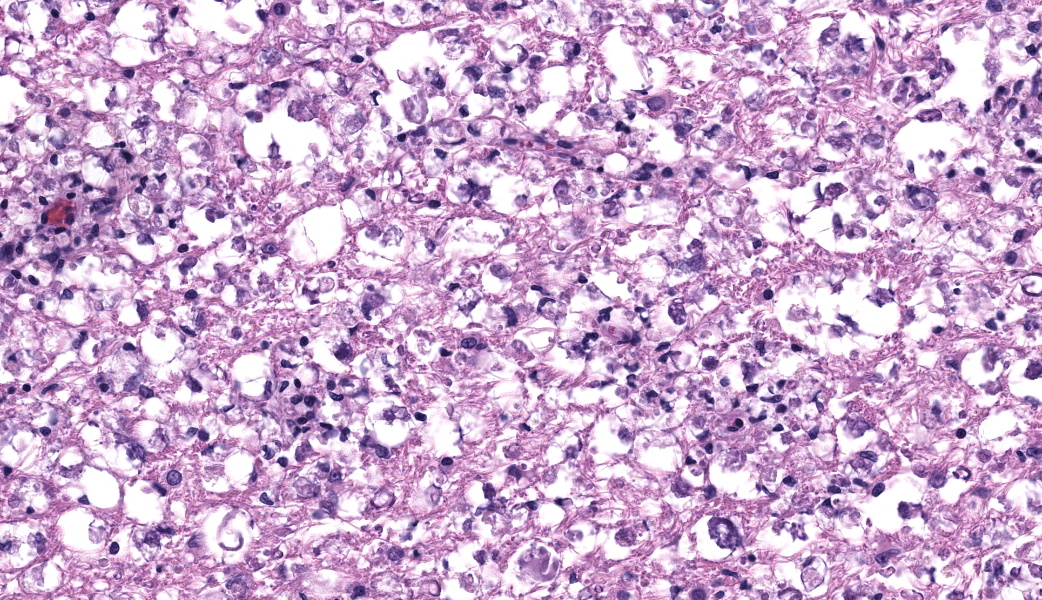
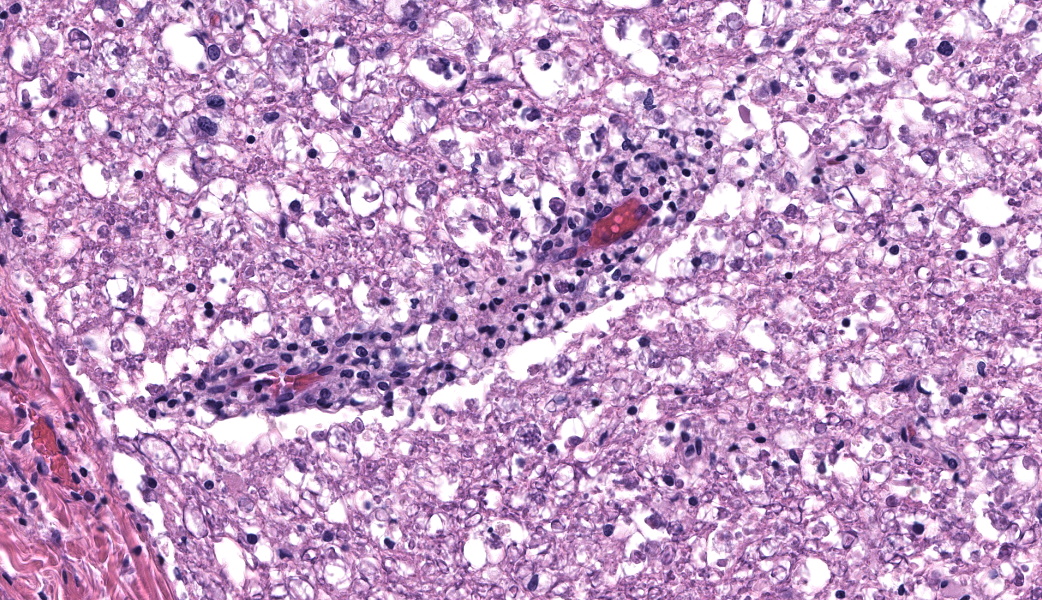
Spinal cord (thoracic segments): In all of the examined cross sections, the white matter of the dorsal funiculi is diffusely and moderately to markedly vacuolated with myelin disruption and loss and axonal degeneration (Wallerian degeneration). Multifocally throughout the white matter of the dorsal funiculi, there are moderately to markedly dilated myelin sheaths, some of which contain gitter cells or eosinophilic cellular debris (ellipsoids); degenerate axons (spheroids); mild to moderate gliosis; and small to moderate numbers of lymphocytes and macrophages. Additionally, there are perivascular cuffs consisting of small numbers of lymphocytes surrounding small- and medium-caliber blood vessels within the dorsal funiculi. These lesions are in marked contrast to the lateral and ventral funiculi, which are within normal limits. There are small numbers of basophilic bacilli scattered throughout all sections (interpreted as postmortem overgrowth/cadaveric bacilli).
Special Stains:
The following special stains were applied to sections of the spinal cord (thoracic segments):
Hematoxylin & eosin/Luxol fast blue: Throughout the dorsal funiculi, there is extensive and marked myelin loss and disruption. These regions contain numerous astrocytes that exhibit haphazard arrangement of the eosinophilic fibrillary acidic proteins of their processes, as well as multifocal accumulations of eosinophilic cellular debris. Extensively scattered throughout the dorsal funiculi, there is rarefaction with vacuolation of the neuropil. Within one of the examined cross sections, there is a dorsal spinal nerve root which exhibits diffuse loss of myelin.
Bielschowsky silver: In all of the examined sections, there is a regionally extensive, marked decrease in axonal density throughout the dorsal funiculi. The axons that remain in this region are frequently shrunken or fragmented.
Contributor's Morphologic Diagnosis:
Spinal cord (dorsal funiculi) - myelin loss and disruption with axonal degeneration (Wallerian degeneration), diffuse, moderate to marked, subacute to chronic, with mild lymphocytic and histiocytic infiltration, lymphocytic perivascular cuffs, and gliosis
Contributor's Comment:
The gross and microscopic lesions observed in this case, particularly the diffuse Wallerian degeneration of the dorsal funiculi throughout the entire length of the spinal cord, are suggestive of canine ganglioradiculitis, also known as sensory neuropathy or sensory neuronopathy. Canine ganglioradiculitis is described as a rare, idiopathic disease of adult dogs characterized by various degrees of inflammation within the peripheral ganglia, dorsal root ganglia, dorsal spinal nerve roots, and dorsal funiculi of the spinal cord.1,3,5-9 On histopathology, the characteristic features of the disease include nonsuppurative inflammation of the dorsal root spinal ganglia and cranial sensory ganglia with secondary, extensive Wallerian degeneration in the dorsal funiculi throughout the entire length of the spinal cord.5 In the case presented here (but not included in the submitted sections), there were variable degrees of mononuclear inflammation, gliosis, myelin loss, and neuronal degeneration within select dorsal nerve roots and dorsal root ganglia; however, the most striking gross and histopathologic lesions involved the dorsal funiculi throughout the entire length of the spinal cord (as exhibited on the submitted slide). These lesions included marked Wallerian degeneration characterized by myelin disruption and loss, with axonal degeneration. Mononuclear infiltration, both in the form of perivascular cuffing as well as throughout the dorsal funiculi, was also an important feature in this case.
Canine ganglioradiculitis has been reported to be a sporadic disease usually affecting adult dogs with no breed or sex predilections.5 This condition is considered a general proprioceptive disorder without involvement of the motor system.3 The clinical signs associated with this condition are usually abrupt in onset and slowly progressive (over several months) and can be asymmetrical. In this case, the dog initially presented with hypermetria of the right forelimb and the signs progressed toward sensory ataxia and a hypermetric gait in all four limbs. The clinical signs of canine ganglioradiculitis are variable, but often include generalized sensory ataxia, hypermetria, base-wide stance, depression or loss of spinal reflexes, reduced postural reactions, facial hypalgesia, dysphagia, masticatory muscle wasting, and megaesophagus.5 Additionally, cerebrospinal fluid findings can be normal or exhibit increases in both cells and proteins, as was reported in this case.8
Hereditary sensory neuropathies have been reported in Long-haired Dachshund dogs and in Pointer dogs.2,4 In the case of Long-haired Dachshunds, the clinical signs include loss or reduction of proprioception, reduced or absent pain sensation, and urinary and fecal incontinence. Histologically, there is a decrease in the number of myelinated nerve fibers in numerous peripheral nerves (including the radial and saphenous nerves) as well as axonal degeneration, particularly of unmyelinated C fibers.4 With Pointer dogs, the condition is clinically characterized by acral mutilation and insensitivity and is histologically characterized by reduction in the number of neurons within ganglia; however, neuronal degeneration and degenerating myelinated axons within the ganglia are considered rare in these cases.2 A decrease in the density of myelinated fibers within the dorsolateral fasciculus of the spinal cord has been associated with the hereditary condition in Pointer dogs.2 An additional clinical differential to be considered is Coonhound paralysis or idiopathic polyradiculitis; however, the pathologic changes of this neuropathy are usually concentrated at the ventral roots and associated clinically with motor deficits such as tetraplegia.5
The cause of canine ganglioradiculitis remains unknown. Hypotheses concerning the cause of this condition include an immune-mediated pathogenesis (with cell-mediated and/or humoral components), a viral infection, or a toxic etiology. Autoantibody detection using indirect immunofluorescence assay on the sera from two dogs did not detect autoantibodies against canine ganglion tissues.5
Contributing Institution:
University of Minnesota Veterinary Diagnostic Laboratory College of Veterinary Medicine 244 VDL, 1333 Gortner Ave. St. Paul, MN 55108 https://www.vdl.umn.edu/
JPC Morphologic Diagnosis:
Thoracic spinal cord, dorsal funiculi: Axonal degeneration and loss, chronic, diffuse, marked, with mild lymphocytic perivascular leukomyelitis.
JPC Comment:
Dr. Jey Koehler, from Auburn University's School of Veterinary Medicine (and our Department consultant on all things neuropathological), moderated this year's 23rd conference with a lineup of neuro cases that integrated anatomy, histology, and clinical neurology. Before diving into this first case, there was a review of the three true forms of ataxia: cerebellar, vestibular, and proprioceptive. Understanding the differences can help clinicians and pathologists localize neurologic disease, and it is common to have more than one type play a role. Cerebellar ataxia is characterized by ataxia and dysmetria or hypermetria of all four limbs, a "goose-stepping" gait, wide-based stance, truncal sway, and intention tremors, but with normal strength and proprioception. Vestibular ataxia can also have a wide based stance, but affected animals have more of a "crab-walking" or "wall-walking" gait, have lateralized lesions (i.e., head tilt, leaning or circling to one side, etc.), falling/stumbling, and a loss of balance when the head is lifted or the eyes are covered. Lastly, animals with a proprioceptive ataxia show scuffing of the toes when walking, knuckling, crossing over of the limbs, truncal sway, "abnormal stance", and exaggerated circumduction, abduction, and adduction. This dog's history suggested combined vestibular and proprioceptive ataxias. In vestibular ataxia, there is a dysfunction of the vestibular reflex pathways that maintain eye, head, and body position, while proprioceptive ataxia is secondary to loss of neural input from proprioceptors (i.e., muscle spindles, ligaments, joint receptors, etc.). This ataxia review emphasized why a good history is crucial for interpretation of neurologic lesions.
Participants were encouraged to always pay attention to neuroanatomic location when evaluating the nervous system and to be as specific as possible. This was a theme that ran through all four cases in this conference, and Dr. Koehler shared tips on how to determine precisely at which level of the spinal cord a particular histology section may have been taken from, based on the shape of the cord, gray-to-white matter ratio, and the presence of specific tracts. The cervical spinal cord characteristically is either top-heavy (especially pronounced at the level of C1) or is symmetrically oval with a high proportion of white matter. She emphasized how caudal cervical and proximal lumbar segments can look deceptively similar on histology, and how careful attention to the dorsal columns, particularly the medially located fasciculus gracilis (pelvic limb input) and more lateral fasciculus cuneatus (thoracic limb input), can help orient the pathologist. She shared a clever mnemonic to make the distinction between their functions memorable: "If you want to be a graceful dancer, you need legs; if you want to write in cuneiform, you need arms."
The thoracic spinal cord, by comparison, is more spherical and has very little grey matter compared to the other segments. Here, there may be lateral horns (intermediate column) that are composed of visceral motor neurons. In the lumbar segment, the spinal cord becomes bottom-heavy with large ventral horns and a dorsal "caterpillar" shape. The lumbar cord also has a higher proportion of grey matter compared to the cervical segment. Lastly, the sacral cord, is comparatively small with a high proportion of grey matter and usually can be relied upon to have several "nerve friends" nearby. As cited by Dr. Koehler during conference, the University of Minnesota's online "Spinal Cord Anatomy Lab" is an excellent resource for learning the distinguishing histologic features of each cord segment.
Then on to this particular case - many of the major features of sensory neuropathy/ganglioradiculitis discussed during conference are covered in the contributor's excellent write-up. One of the central discussions during this case was whether it should be given a morphologic diagnosis of leukomyelitis, axonal degeneration, or as demyelination. The inflammation in this particular section was minimal, leading some participants to balk at the idea of using the "-itis" terminology. Dr. Koehler emphasized that, while she views this condition as fundamentally inflammatory since current literature points to the pathogenesis likely being immune-mediated with predominant T-lymphocyte infiltrates, this case lacked the histologic features necessary to truly label it as leukomyelitis.7 Additionally, inflammation in cases of sensory neuropathy is often minimal in the cord itself, but may be prominent in the dorsal ganglia.7 As such, the primary lesion is thought to occur in the ganglia with secondary degeneration of the central projections in the dorsal columns.7 Without the dorsal root ganglia in section, the group was left to interpret the pattern of a disease restricted to the ascending sensory tracts (white matter), with Wallerian-like degeneration.6,7 This was reflected in the JPC's morphologic diagnosis, which prioritized the axonal degeneration and loss as the primary process in this slide, with a secondary leukomyelitis.
References:
- Cantile C, Youssef S. Nervous System. In: Maxie MG, ed. Jubb, Kennedy, and Palmer's Pathology of Domestic Animals. Vol. 1. 6th ed. St. Louis, MO: Elsevier; 2016:395.
- Cummings JF, de Lahunta A, Winn SS. Acral mutilation and nociceptive loss in English pointer dogs. Acta Neuropathol. 1981;53(2):119-127.
- De Lahunta A, Glass E, Kent M. Veterinary Neuroanatomy and Clinical Neurology. St. Louis, MO: Elsevier Saunders; 2015:252-253.
- Duncan ID, Griffiths IR, Munz M. The pathology of a sensory neuropathy affecting Long haired Dachshund dogs. Acta Neuropathol. 1982;58(2):141-151.
- Funamoto M, Nibe K, Morozumi M, et al. Pathological features of ganglioradiculitis (sensory neuropathy) in two dogs. J Vet Med Sci. 2007;69(12):1247-1253.
- Hamzianpour, N, Eley, TS, Kenny, PJ, et al. Magnetic resonance imaging findings in a dog with sensory neuronopathy. J Vet Intern Med. 2015;29(5):1381-1386.
- Porter B, Schatzberg S, McDonough S, et al. Ganglioradiculitis (sensory neuronopathy) in a dog: Clinical, morphologic, and immunohistochemical findings. Vet Pathol. 2002;39(5):598-602.
- Summers BA, Cummings JF, de Lahunta A. Veterinary Neuropathology. St. Louis, MO: Mosby-Year Book, Inc; 1995.
- Wouda W, Vandevelde M, Oettli P, et al. Sensory neuronopathy in dogs: A study of four cases. J Comp Pathol. 1983;93(3):437-450.