Joint Pathology Center
Veterinary Pathology Services
Wednesday Slide Conference
2017-2018
Conference 1
August 23rd, 2017
CASE I: 11-1259-7 (JPC 4017218).
Signalment: Ten-year-old, castrated male, mixed breed canine (Canis lupis familiaris).
History: A reportedly 10 year old male castrated mixed breed dog presented for complete necropsy following euthanasia. The dog had a three week history of lethargy, weakness, dyspnea, tachypnea and in-appetence. There was a history of a left total hip replacement and bilateral hip dysplasia. The dog had been on Deramaxx since 2003 and Tramadol since 2009. On presentation the dog was in respiratory distress with a heart rate of 180 bpm. There was pitting edema in the right front forelimb.
Gross Pathology: The dog had a body condition score of 5/5 and was in good post mortem condition. A firm, red, 1cm diameter mass was present on the dorsal antibrachium, and a soft, 7cm x 4cm white subcutaneous mass was present in the right axillary region (lipoma). The pleural cavity contained approximately 150ml of thin red fluid. Within the cranial mediastinum there was a 30 cm x 26 cm by 15 cm lobulated, poorly demarcated, white to yellow firm mass. On cut surface >75% of the mass was soft and yellow to light green (necrosis). The mass extended into the pericardium and similar masses were present within the right and left atria and auricles, and right ventricular free wall (ranging from 3-6cm in diameter). A single 2-3 cm diameter mass was present within the right cranial lung lobe, and another single 2-3 cm mass was present within the wall of the esophagus. There were multiple masses (1-4cm in diameter) within the wall of the stomach.
Gross Morphologic Diagnosis: None provided.
Laboratory results: None provided.
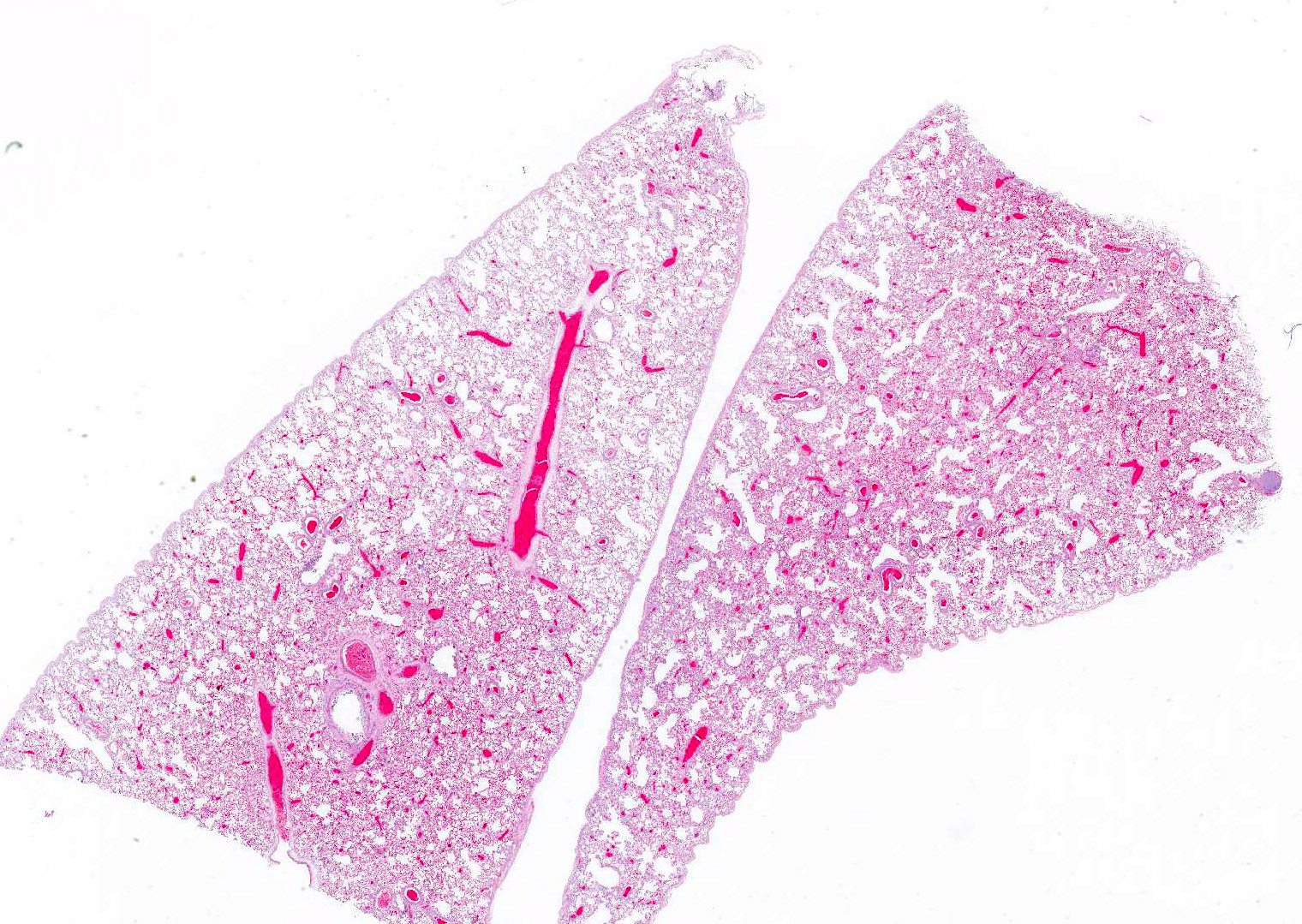
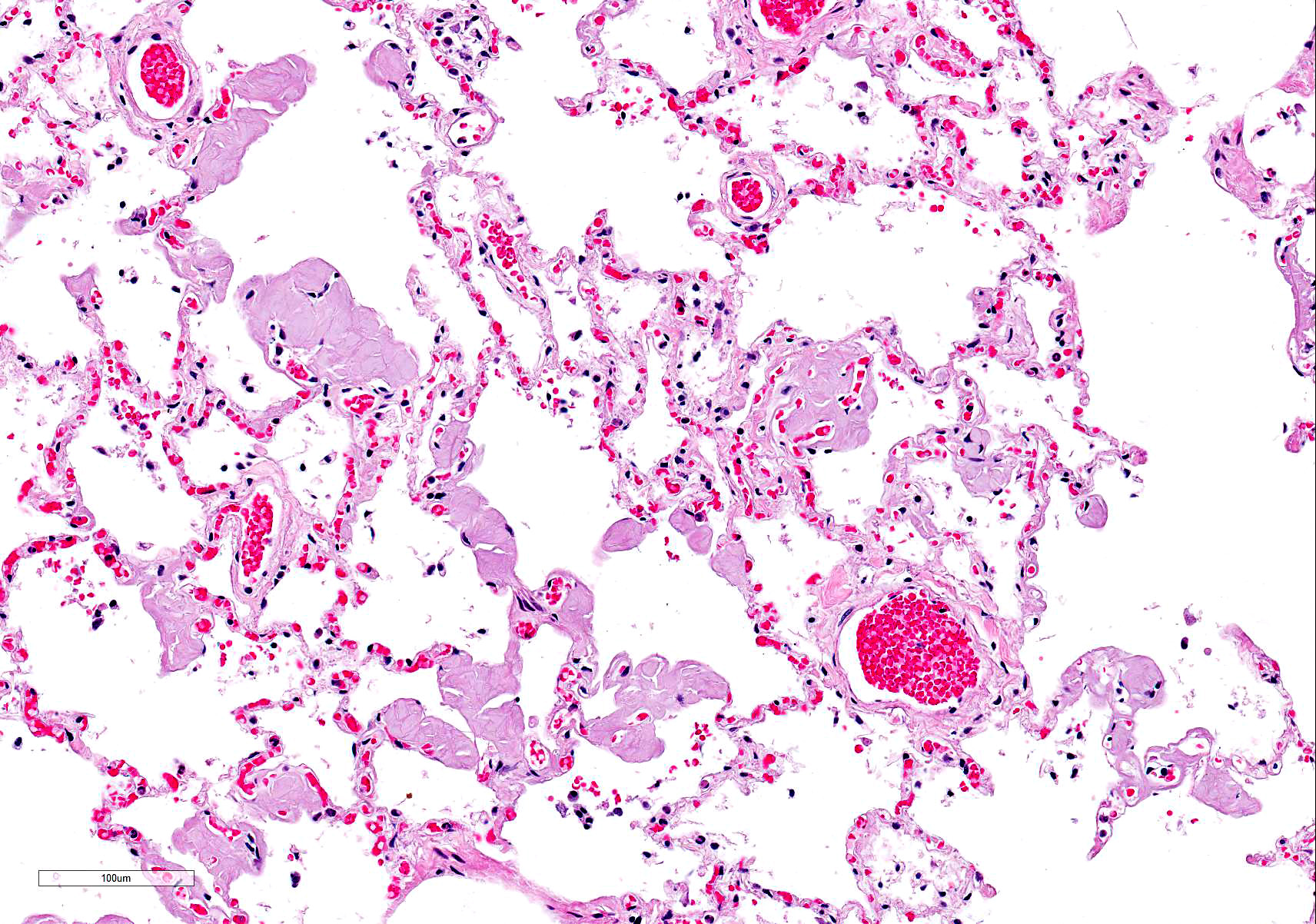
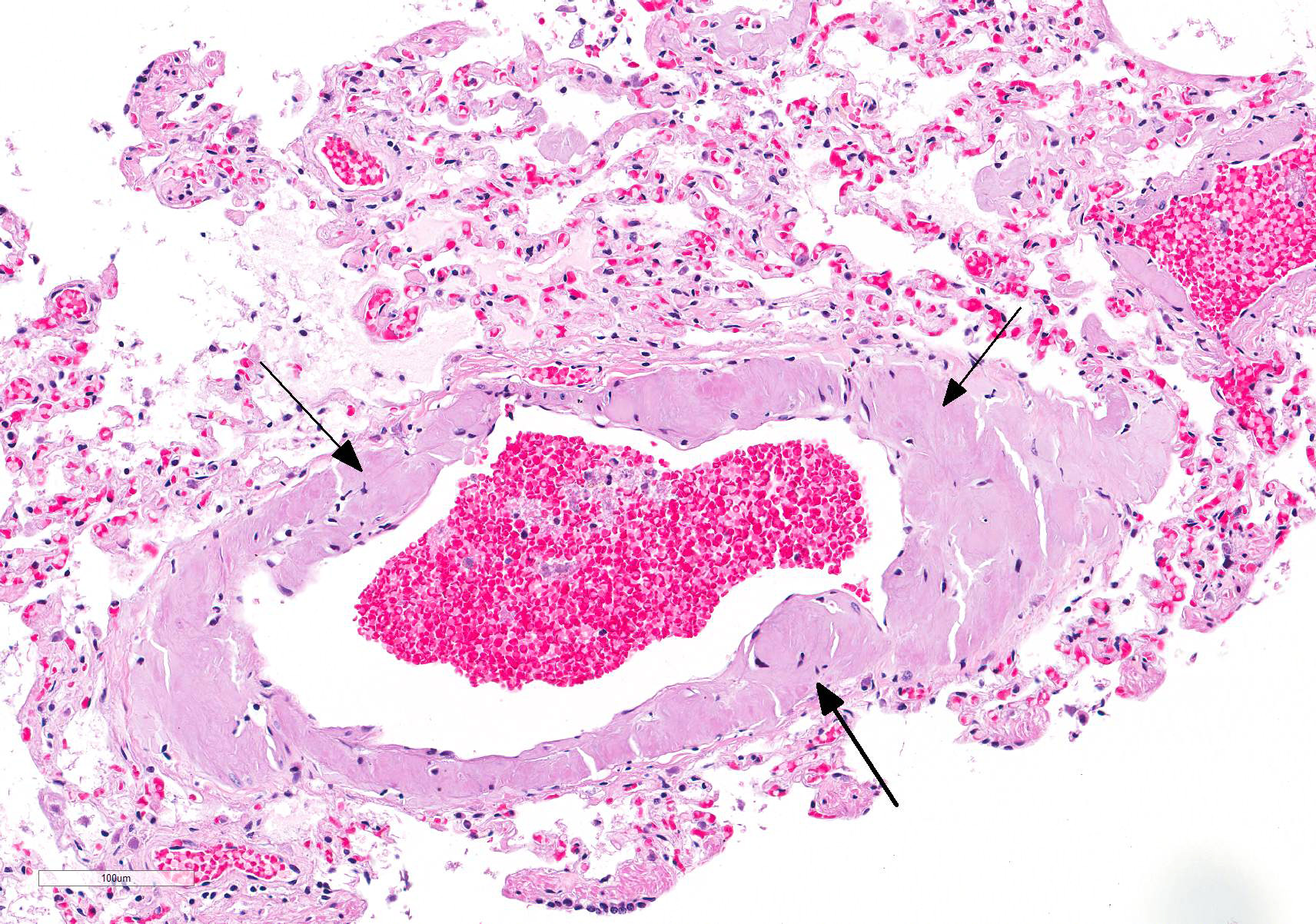
Microscopic Description: Lung: The alveolar interstitium is randomly effaced and expanded by variably sized aggregates of amorphous homogenous eosinophilic material. In addition, similar aggregates are observed replacing the tunica media of pulmonary arteries and arterioles and occasionally of veins. The material can be also seen rarely ruptured into the alveolar air space. Occasionally, organized accumulations of fibrin, neutrophils and erythrocytes are present in arteries and arterioles which are adhered to the endothelial surface of the vessel (thrombosis). Some thrombi contain a flattened cell population adhered to the surface (endothelialization). A moderate multifocal alveolar histiocytosis is present characterized by intra-alveolar accumulations of macrophages with abundant eosinophilic vacuolated cytoplasm. Extramedullary hematopoiesis is present.
Contributors Morphologic Diagnoses: Marked multifocal pulmonary amyloidosis characterized by deposition in arterioles and interstitium with fibrin thrombi, and mild to moderate pulmonary edema.
Contributors Comment: Amyloid is composed insoluble protein arranged in ?-pleated sheets of protein. The conformation of the protein is the primary characteristic responsible for the binding and staining of the Congo red dye. Amyloid is most commonly classified as secondary or AA and primary or AL in veterinary medicine. AA amyloid is associated with chronic inflammation and is composed of fragments derived from serum amyloid A, a serum apolipoprotein and acute phase protein produced by hepatocytes. Familial amyloidosis in the Shar-Pei dog breed and cat breeds such as the Abyssinian and Siamese is also AA amyloid. AL amyloid is formed from immunoglobulin light chains, predominantly ? light chain fragments. This type of amyloid is commonly associated with plasma cell dyscrasias. A? (?-amyloid) is angiocentric cerebral deposits of amyloid recognized in the human and canine. Amyloidosis is also classified as localized or systemic with systemic involvement representing more than 60% of cases (1).
Amyloidosis is reported in several organs in species of veterinary importance but most commonly deposits in the glomerular tuft and peritubular interstitium of the kidney, the periarteriolar lymphoid sheaths in the spleen and the space of Disse in the liver.
Pulmonary amyloidosis is reported in canines and humans. Radiographically, human parenchymal amyloidosis is divided into a nodular form and a diffuse septal form (1). In canines, amyloid deposition in the tunica intima and media of large pulmonary arteries is described. This particular deposition of amyloid is derived from apolipoprotein AI and may be a age related change (2,3). The type of amyloid present in this case was not determined.
JPC Diagnosis: Lung: Amyloidosis, arteriolar, arterial, and interstitial, multifocal, marked with alveolar edema, mixed breed, canine.
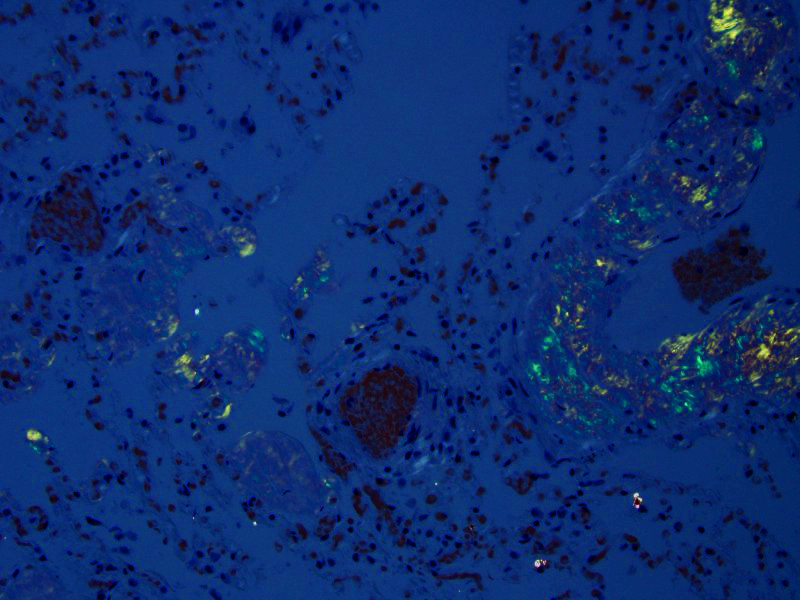
Conference Comment: This case nicely demonstrates the histologic changes associated with pulmonary amyloidosis. A Congo red was run to highlight the apple green birefringence of the deposited amyloid and participants discussed the use of Thioflavine T viewed under a ultraviolet light as an additional amyloid marker.3 Although the microscopic appearance is characteristic, a differential diagnosis of pulmonary arteriolar/arterial and interstitial hyalinosis was discussed. Pulmonary hyalinosis has been reported as a finding in the pulmonary artery of older dogs.10 Hyalinosis can be differentiated from amyloid using periodic-acid shift (PAS) stain which highlights the glassy eosinophilic material.2 The following chart was used to review the classification of different types of amyloidosis:
|
Clinicopathologic Category |
Associated Diseases |
Major Fibril Protein |
Precursor Protein |
|
Systemic (Generalized Amyloidosis) |
|||
|
Primary Amyloidosis (Immune dyscrasias) |
Monoclonal plasma cell proliferations |
AL (Light chain amyloid) |
Ig light chains (mainly ? type, but also ? type) |
|
Secondary Amyloidosis (Reactive systemic amyloidosis) |
Chronic inflammatory conditions |
AA (Amyloid associated) |
SAA (Serum associated amyloid) |
|
Hereditary Amyloidosis |
|||
|
Familial amyloidosis |
Renal impairment |
AA |
SAA |
|
Localized Amyloidosis |
|||
|
Islet amyloid |
Type 2 diabetes mellitus |
AIAPP |
Islet amyloid polypeptide |
|
Cerebral (senile) amyloid |
Cognitive disorder |
A? (Beta-amyloid protein) |
APP (amyloid precursor protein) |
|
Pulmonary vessel amyloid |
? |
Apolipoprotein A-I (apoA-I) |
? |
Chart adapted from table 6-17 in Robbins and Cotran Pathologic Basis of Disease, page 258
While reviewing the chart above, participants were reminded that familial amyloidosis occurs in Shar-Pei dogs and Abyssinian cats with AA amyloid deposition in the renal interstitium as opposed to the glomeruli. In these cases, renal impairment is generally mild and amyloid is usually diagnosed incidentally during necropsy.7
In addition, conference participants discussed the gross appearance of organs containing amyloid deposits as yellow, waxy, coalescing, nodular amorphous deposits that turns brown when stained with Lugols iodine and deep purple with acetic acid.7
Finally, the conference moderator emphasized (as did the contributors in the above comment) that in most domestic species AA amyloid deposition in the liver begins in the space of Disse with the exception of the mouse where deposition occurs in the periportal regions of the liver.1
Contributing Institution:
Department of Veterinary Biosciences
College of Veterinary Medicine
The Ohio State University
http://vet.osu.edu/biosciences
References:
1. Barthold SW, Griffey SM, Percy DH. Mouse. In: Pathology of Laboratory Rodents and Rabbits. 4th ed. West Sussex, UK: Wiley & Sons, Inc.; 2016:92.
2. Cianciolo RE, Mohr FC. Urinary system. In: Maxie MG, ed. Jubb, Kennedy, and Palmers Pathology of Domestic Animals. Vol. 2. 6th ed. London, UK: Saunders Elsevier; 2016:406.
3. Cullen JM, Stalker MJ. Liver and biliary system. In: Maxie MG, ed. Jubb, Kennedy, and Palmers Pathology of Domestic Animals. Vol. 2. 6th ed. London, UK: Saunders Elsevier; 2016:279.
4. Johnson KH, Sletten K, Hayden DW, O"Brien TD, Roertgen KE, Westermark P. Pulmonary vascular amyloidosis in aged dogs. A new form of spontaneously occurring amyloidosis derived from apolipoprotein AI. Am J Pathol. 1992 Nov;141(5):1013-9.
5. Kumar V, Abbas AK, Aster JC. Diseases of the immune system. In: Robbins and Cotran Pathologic Basis of Disease. 9th ed. Elsevier Saunders; 2015: 256-262.
6. Lachmann HJ, Hawkins PN. Amyloidosis and the lung. Chronic Respiratory Disease. 2006;3(4):203-14.
7. Miller MA, Zachary JF. Mechanisms and morphology of cellular injury, adaptation, and death. In: McGavin MD and Zachary JF, eds. Pathologic Basis of Veterinary Disease. 6th ed. Elsevier, Mosby Saunders; 2016: 30-31.
8. Roertgen KE, Lund EM, O"Brien TD, Westermark P, Hayden DW, Johnson KH. Apolipoprotein AI-derived pulmonary vascular amyloid in aged dogs. Am J Pathol. 1995 Nov;147(5):1311-7.
9. Snyder PW. Diseases of immunity. In: McGavin MD and Zachary JF, eds. Pathologic Basis of Veterinary Disease. 4th ed. Elsevier, Mosby Saunders; 2007: 1488.
10. Williams, K. Coronary arteriosclerosis with myocardial atrophy in a 13-year-old dog. Veterinary Pathology. 2003 Nov; 40(6), 695-697.
11.