WSC 2023-2024, Conference 14, Case 2
Signalment:
10-year-old, intact female Tennessee Walking Horse (Equus caballus)
History:
The patient had a history of a mass in the nose and troubled breathing. A mass was confirmed on radiographs and via endoscopic examination.
Gross Pathology:
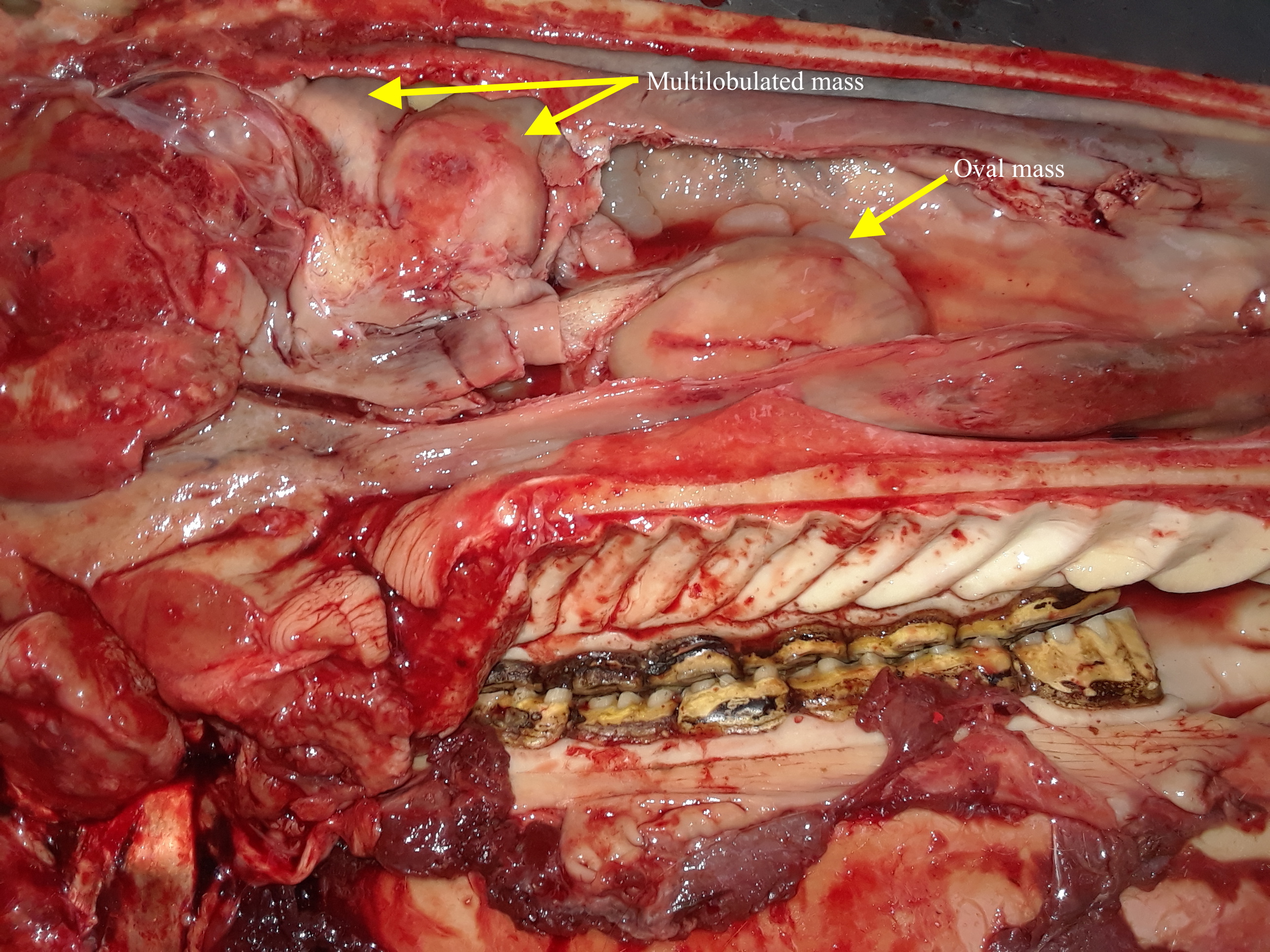
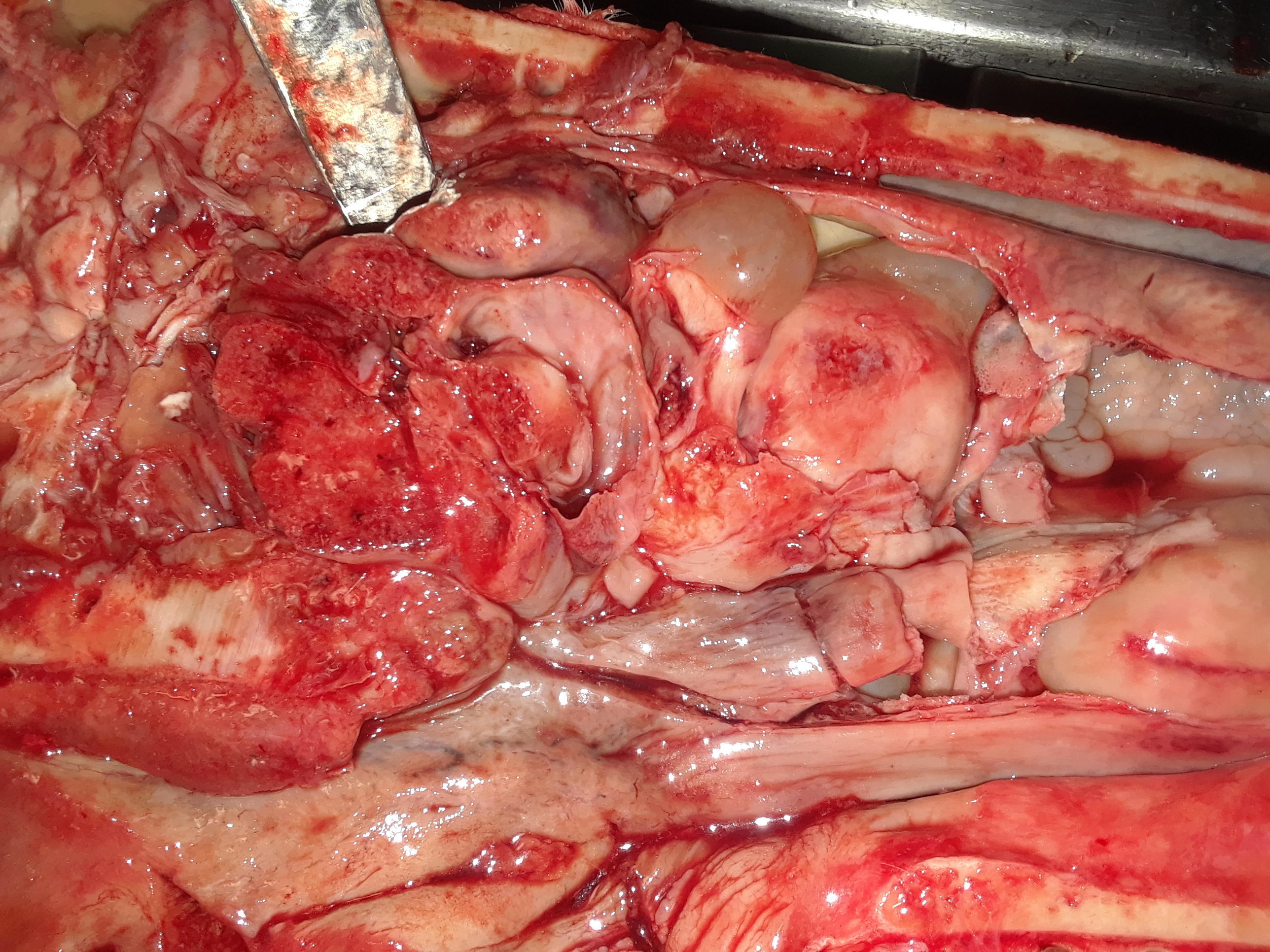
The carcass was in adequate body condition (5.5/9). A mild creamy yellow viscous mucus-like nasal discharge was present. Saggital sectioning of the head revealed multiple firm to hard cream-colored masses. In the ventral nasal concha there was an oval 7 cm x 4 cm x 2 cm mass with a linear cobblestone appearance in the rostral aspect of the mass. Invading the dorsal concha was another irregular multilobulated mass, measuring 5.5 cm x 4 cm x 5 cm, which contained several tan to gray soft, rounded cyst-like fluid-filled structures. The left ethmoid turbinates contained a similar 5 cm x 5 cm mass.
On the surface of the right caudal lung lobe at the caudal border, there was a 6.5 cm x 7 cm, slightly elevated, cream-colored, gelatinous, irregular, focally extensive area with short thick projections. The surface of these projections had multifocal to coalescing pinpoint to 2 cm red foci, and cut section of this area revealed two round, semi-firm, opaque yellow nodules that extended 1 cm into the lung parenchyma. Twelve centimeters cranially to the aforementioned lesion there was another similar (cream colored, gelatinous with pinpoint red discolorations) area measuring 1 cm x 0.5 cm.
Microscopic Description:
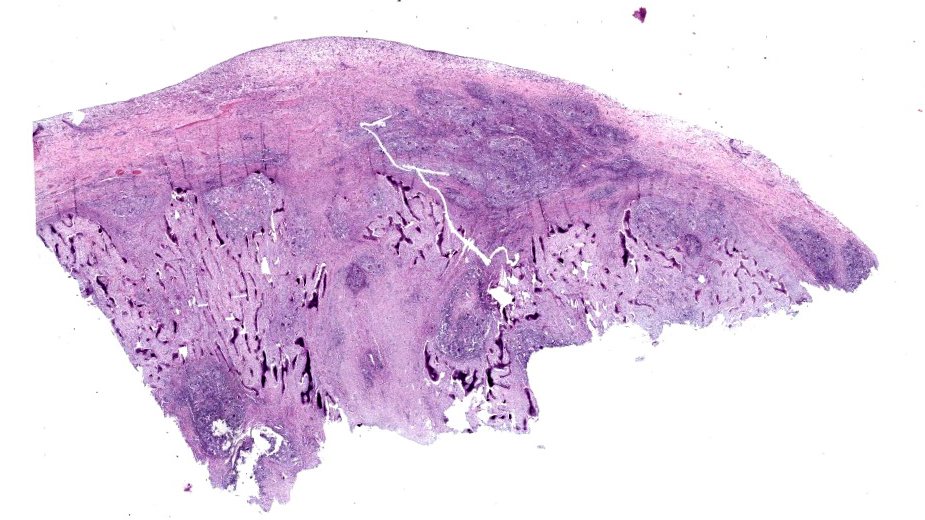
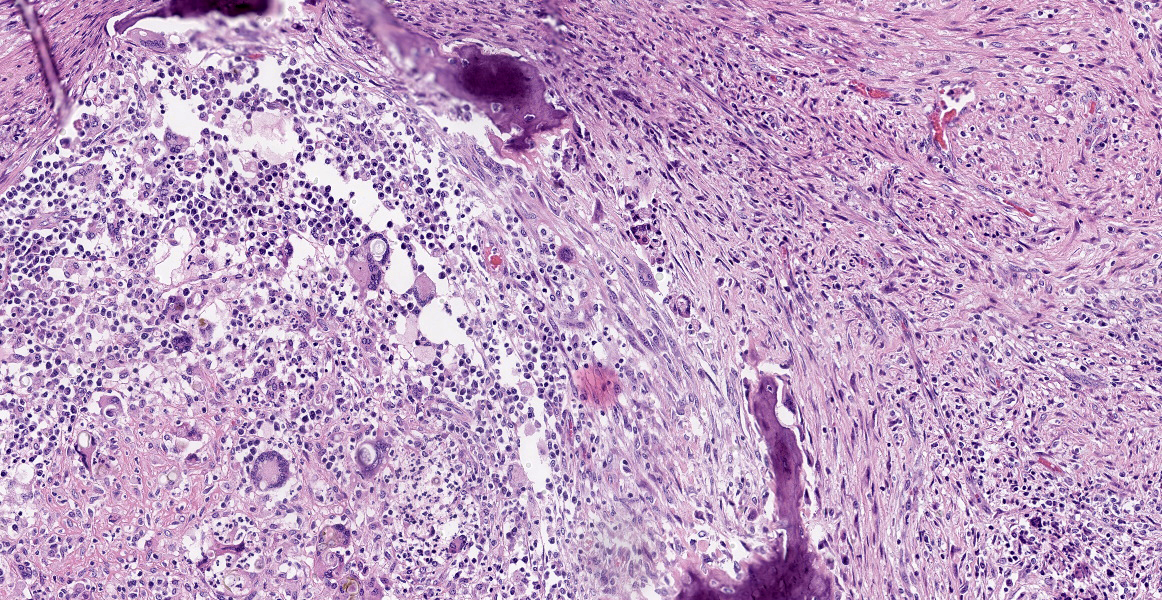
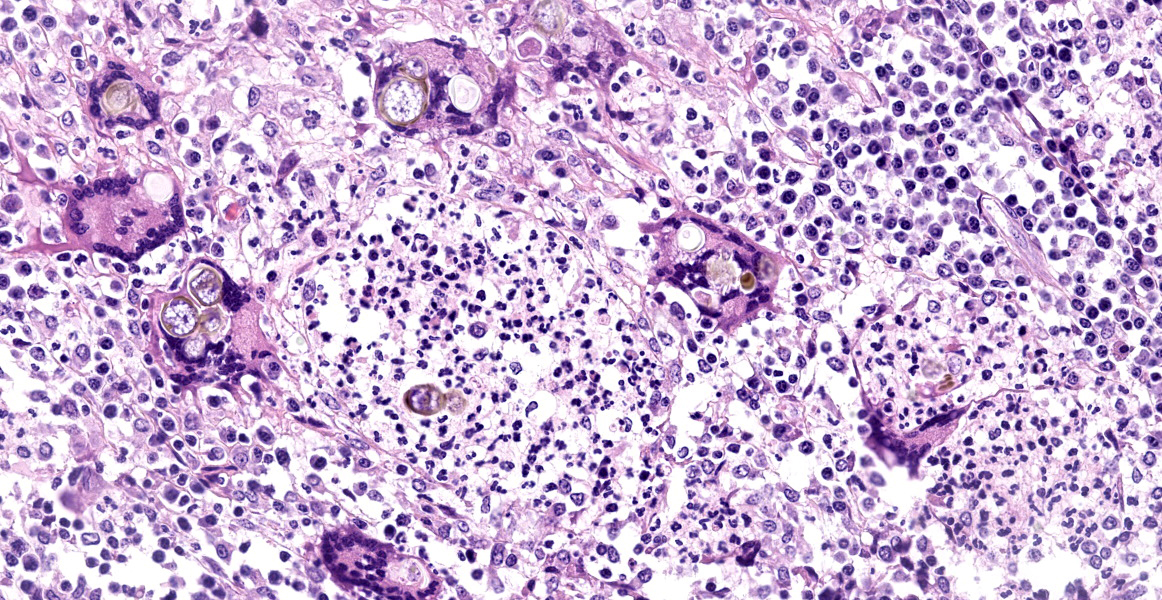
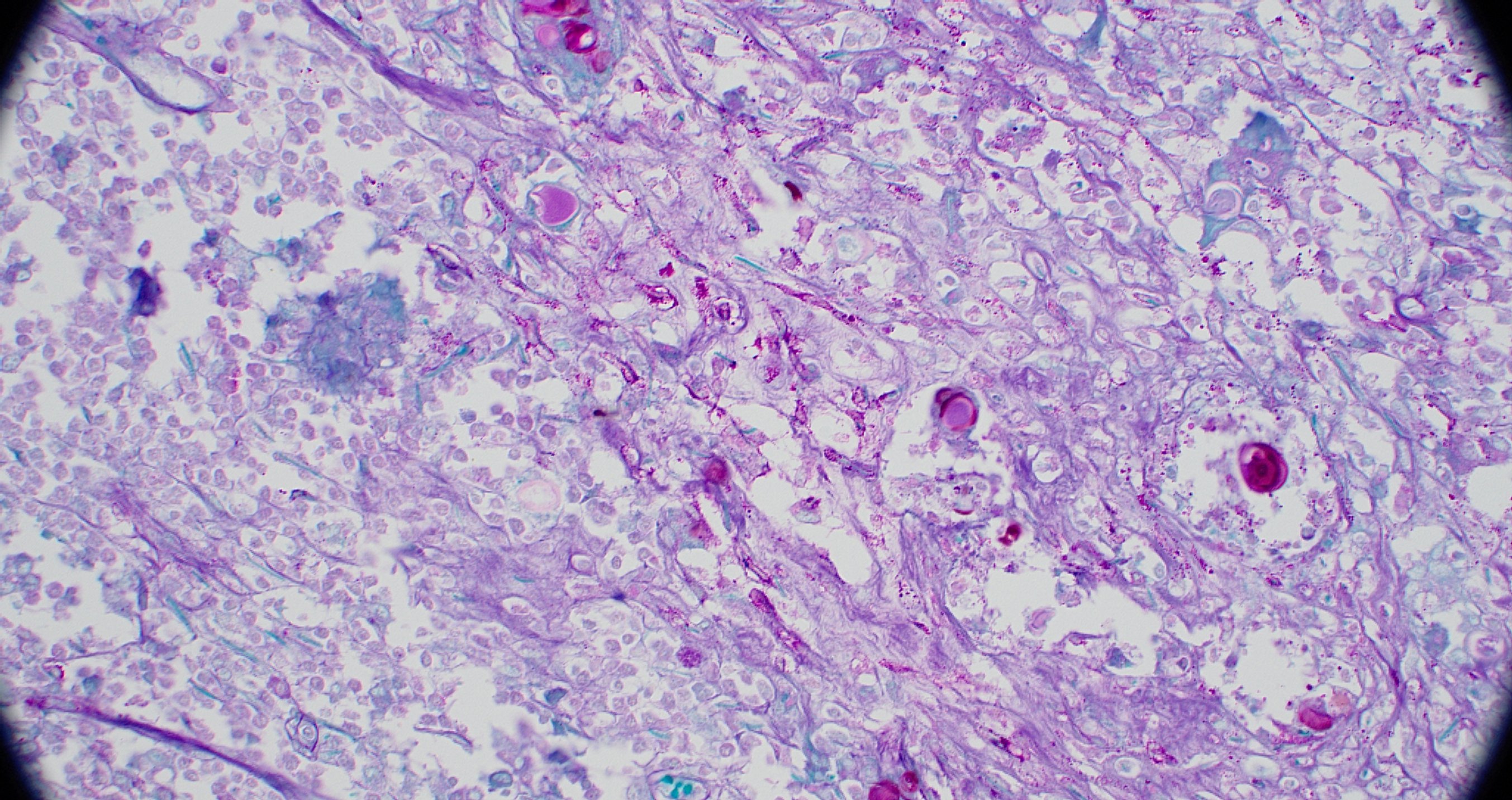
Nasal turbinates: Infiltrating and effacing >90% of the nasal turbinates are multifocal to coalescing nodular foci of inflammation centered on myriad dematiaceous mycotic agents.The inflammation consists of numerous macrophages with Langhans and foreign body type macrophages, numerous plasma cells, fewer lymphocytes, and random aggregates of neutrophils, which are surrounding numerous round to oval, 30-60 µm spherules with a 2-3 µm clear to brown stained capsule. These structures are frequently filled with several 3-6 µm clear to lightly basophilic rounded structures that are clustered together. The mycotic agents are frequently within multinucleated giant cells. Rarely, the organisms form 5-6 µm septate hyphae which were observed with Periodic Acid-Schiff (PAS) stain.
Contributor’s Morphologic Diagnosis:
Nasal cavity: Severe multifocal granulomatous rhinitis with intralesional dematiaceous fungi (Phaeohyphomycosis).
Contributor’s Comment:
On macroscopic examination it was thought that the lesion in the nose was a neoplastic process; however, histologic examination revealed the presence of dematiaceous (pigmented) mycotic agents associated with a granulomatous inflammatory process.
Dematiaceous fungi are naturally pigmented molds whose hyphae and conidia contain melanin.2 They are ubiquitous and can be found in soil, plants, and organic debris.2
Melanin is what gives the dematiaceous fungi their pigmentation and it is believed to contribute to the organism’s ability to elude the host immune response.5,6 Melanin contributes to the evasion of the immune response by blocking the effects of hydrolytic enzymes on the cell wall and scavenging free radicals released by phagocytic cells during the oxidative burst.6 There are several clinical presentations of dematiaceous molds, including eumy-cetoma, chromoblastomycosis,and phaeohyphomycosis. Our case is an example of phaeohyphomycosis.
Phaeohyphomycosis is an infection caused by dematiaceous (pigmented) fungi which typically affects immunocompromised individuals, but can also affect those that are immunocompetent.2,5 Clinically, infections range from superficial colonization to systemic abscess formation and dissemination.6 The fungi can be unicellular as well as yeast-like, but the key feature is the melanin pigment which distinguishes them from other fungi that may have similar morphology.6 There are many causes of phaeohyphomycosis; the ones most commonly reported in equines are Alternaria sp., Dreschslera sp., and Curvularia sp.1
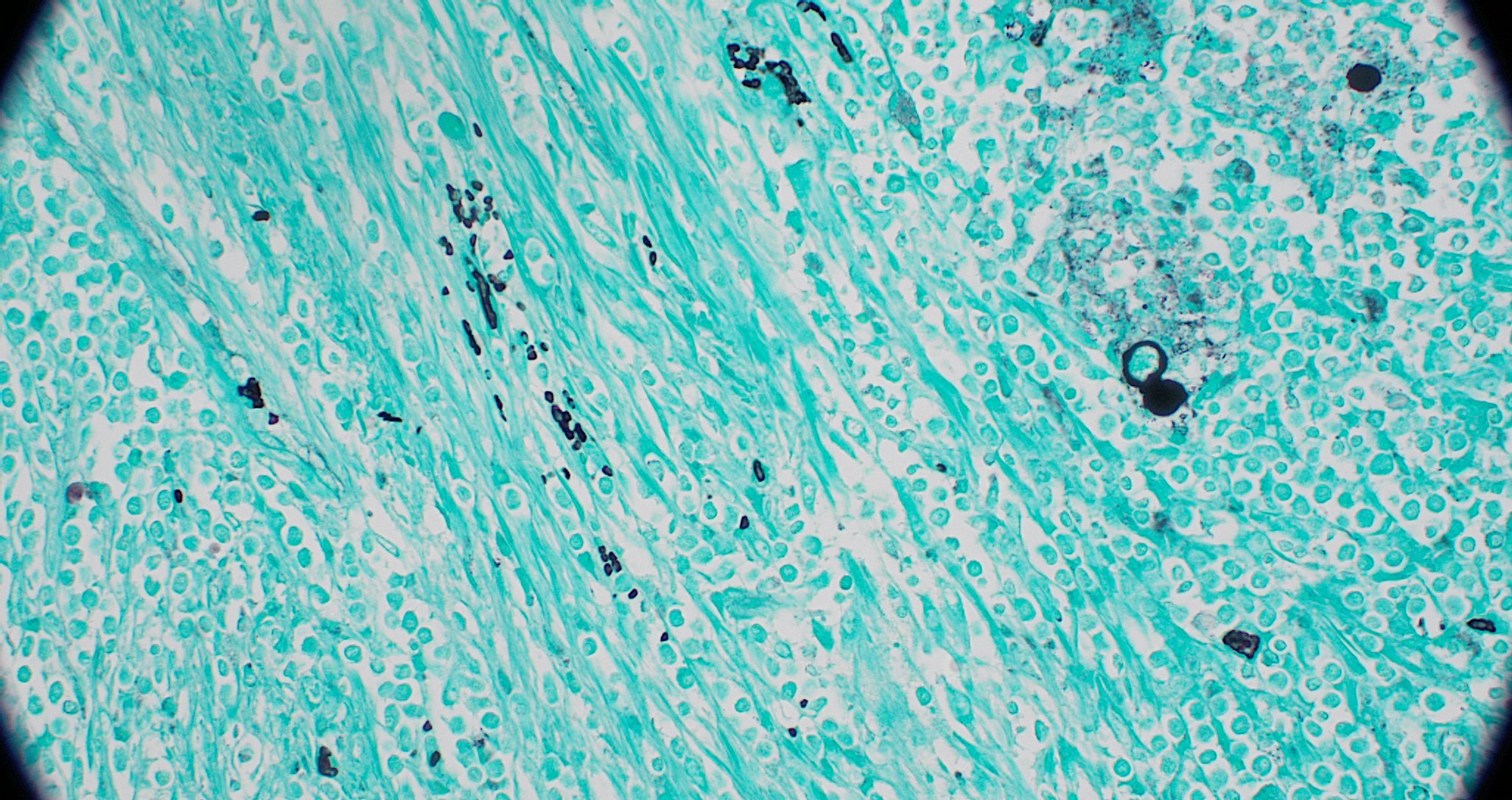
The presence of pigmentation on histopathology warrants a diagnosis of phaeohyphomycosis. In cases with dematiaceous fungi that are poorly pigmented, Fontana-Masson can be used to accentuate the melanin.5 As with other mycotic agents, Periodic Acid-Schiff (PAS) and Grocott-Gomori methenamine silver (GMS) are common stains used to visualize the agents. Culture as well as molecular analysis can also be used to further narrow the identification down to the species level.6
Contributing Institution:
Tuskegee University
College of Veterinary Medicine
Department of Pathobiology, https://www.tuskegee.edu/programs-courses/colleges-schools/cvm
JPC Diagnosis:
Nasal mucosa: Rhinitis, granulomatous, multifocal to coalescing, severe, with turbinate bone lysis and numerous pigmented fungal yeast-like cells and hyphae.
JPC Comment:
This case provides both an excellent example of dematiaceous fungi and a reason to revisit the various classifications of cutaneous fungal infections, particularly in light of an excellent, recently published review article on the subject.3
In general, cutaneous infection with opportunistic fungi presents as nodules or masses in the dermis and/or subcutis which may become ulcerated and develop draining tracts.3 Histologically, fungal lesions are typically characterized by pyogranulomatous or granulomatous inflammation; some fungal infections may have a significant eosinophilic component, depending on species.3 Fungi generally grow as hyphae in tissue and can be demonstrated by PAS and GMS stains to highlight histomorphologic features useful in narrowing differential diagnoses.3
Infection with non-dermatophytic, non-dimorphic, nonpigmented saprophytic fungi that
grow as hyphae in tissue is referred to broadly as hyalohyphomycosis. Note that Aspergillus sp., fungi of the order Mucorales, and Conidiobolus spp and Basidiobolus spp, the agents of entomophthoromycosis, while all nonpigmented hyphae-forming fungi, are typically categorized separately from general hyalohyphomycosis.3
Phaeohyphomycosis refers to infection with pigmented saprophytic fungi that grow as hyphae and yeast-like cells in tissue. The term chromoblastomycosis is used for infection with a subset of pigmented fungi that predominately form large, round, thick-walled cells with prominent septations, called sclerotic bodies or Medlar bodies.3 While small numbers of hyphae may be observed in chromoblastomycosis, sclerotic bodies are the predominant fungal form in the lesion.3 Note that, as in this case, phaeohymphocosis may contain yeast-like cells; these may be differentiated from the sclerotic bodies of chrombolastomycosis by their thinner walls, septations in a single plane, and typical arrangement in chains.3
|
Agent Category |
Description |
Representative Species |
|
White-grain eumycotic mycetoma |
|
|
|
Black-grain eumycotic mycetoma |
|
|
|
Hyalohyphomycosis |
|
|
|
Phaeohyphomycosis |
|
|
|
Chromoblastomycosis |
|
|
|
Entomophthoromycosis |
|
|
|
Table 2-1. Selected organisms causing dermal to subcutaneous fungal infections in animals. Adapted from Hoffman, et al. Vet Pathol. 2023;60(6):814.3 |
||
It is unknown what factors cause a particular fungus to cause phaeohyphomycosis versus chromoblastomycosis, though most cases of chromoblastomycosis in veterinary medicine have been described in amphibians and horses.3
Separate from the categorization of pigmented vs. non-pigmented fungi is the clinical presentation referred to as mycetoma. A mycetoma is a dermal and/or subcutaneous nodule with three typical features: swelling, an exudate containing grossly apparent grains or granules that represent large aggregates of the infectious agent, and a draining tract.3 Mycetomas are divided into those caused by bacteria (termed actinomycotic mycetomas) or fungi (eumycotic mycetomas). Eumycotic mycetomas may be further subdivided into black-grain eumycotic mycetomas and white-grain eumycotic mycetoma, depending on whether they are caused by pigmented or non-pigmented fungi, respectively.3 Confusingly, eumycotic mycetoma is a morphologic classification that is not based on the inciting organism, so the same fungal species that may cause hyalohyphomycosis or phaeohyphomycosis may alternatively cause eumycotic mycetomas if tissue grains are present.3 Common representative species of each of the categories discussed above are presented in Table 2-1.
Participants discussed the yeast-like cells present throughout the section and considered a diagnosis of chromoblastomycosis given the prominence of the yeast-like cells on H&E section; however, PAS staining revealed numerous hyphae and participants noted that the yeast-like cells are frequently arranged in chains, making phaeohyphomycosis the appropriate diagnosis. Participants also discussed the arrangement and character of the bone present in section, particularly the arrangement of the bone fragments perpendicular to the nasal mucosa. Participants felt that the bony fragments represent periosteal new bone growth rather than lysed turbinates, which be oriented parallel to the mucosal surface. Participants felt that the turbinates have been destroyed completely by this inflammatory process, leaving behind only remodeling woven bone. The morphologic diagnosis retains the emphasis on bony lysis, though, in the examined section, we are left with only its aftermath to appreciate.
References:
- Cafarchia C, Figueredo LA, Otranto D. Fungal diseases of horses.Veterinary Microbiology. 2013:215-234.
- Guarner J, Brandt ME Brandt. Histopathologic diagnosis of fungal infections in the 21st century. Clinical Microbiology Reviews. 2011:247-280.
- Hoffman AR, Ramos MG, Walker RT, Stranahan LW. Hyphae, pseudohyphae, yeasts, spherules, spores, and more: A review on the morphology and pathology of fungal and oomycete infections in the skin of domestic animals. Vet Pathol. 2023;60(6):812-828.
- Mauldin EA, Peters-Kennedy J. Integ-umentary System. In: Maxie G, ed. Jubb, Kennedy and Palmer`s Pathology of Domestic Animals. 6th ed. Vol 1. Elsevier; 2016.
- Pumlee Q, Meason-Smith C, Dieterly A, et al. Chaetomiaceae fungi, novel pathogens of equine neurotropic phaeohyphomycosis. Vet Pathol. 2017;54(5):813-819.
- Seyedmousavi S, Guillot J, de Hoog GS. Phaeohyphomycoses, emerging opportunistic diseases in animals. Clin Microbiol Rev. 2013;26(1):19-35.