Conference 23
CASE IV:
Signalment:
5-year-old female spayed Blue Heeler Mix, Canis lupus familiaris, Canine.
History:
The patient had a two-week history of progressive clinical signs, initially presenting with bilateral elevation of the third eyelids, corneal ulcer in the right eye, coughing, leaving the tongue out of the mouth, and declining demeanor. Upon presentation to Colorado State University Urgent Care Service for evaluation of dysphagia and lethargy, dull mentation was noted. Neurological examination revealed absent palpebral and menace responses, as well as absent nasal sensation bilaterally. A negative direct and consensual pupillary light reflex was noted in the right eye. Due to quality-of-life concerns and an uncertain prognosis, humane euthanasia was elected.
Gross Pathology:
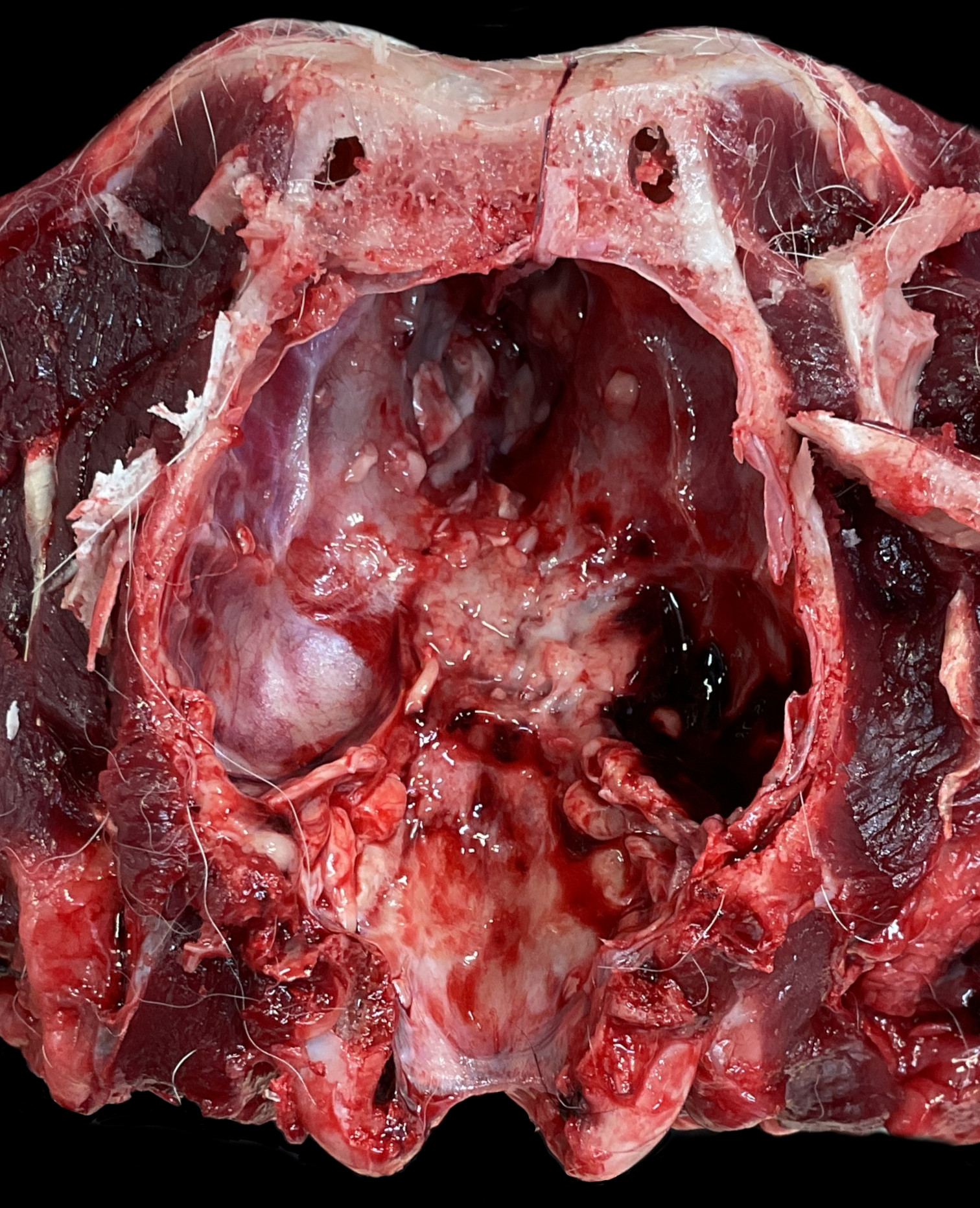
Along the ventral aspect of the brain, obscuring the optic nerve and pituitary gland, is a poorly demarcated region of soft white material surrounded by hemorrhage. Similar material is identified filling the sella turcica and extending along the right caudal cranial fossa and sellar region.
On the right eye there is a focal, centrally located, corneal ulcer measuring approximately 5mm X 3mm. Within the oral cavity, along the caudal right buccal mucosa there are multiple regions of ulceration, which sometimes align with adjacent dentition, ranging in size from 0.5cmX0.9cm to 0.7cmX1.2cm.
Laboratory Results:
Not performed.
Microscopic Description:
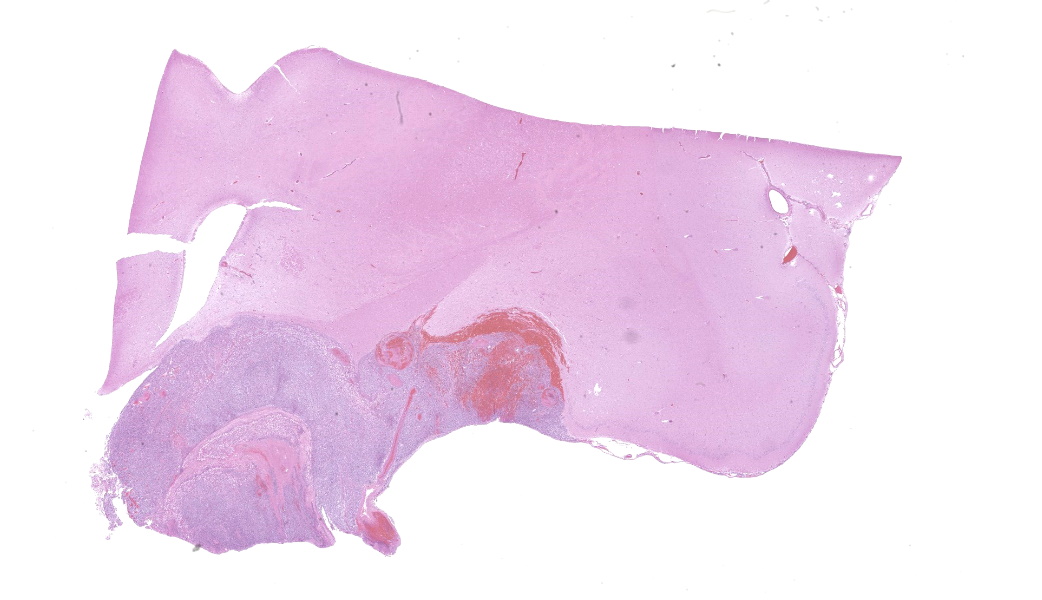
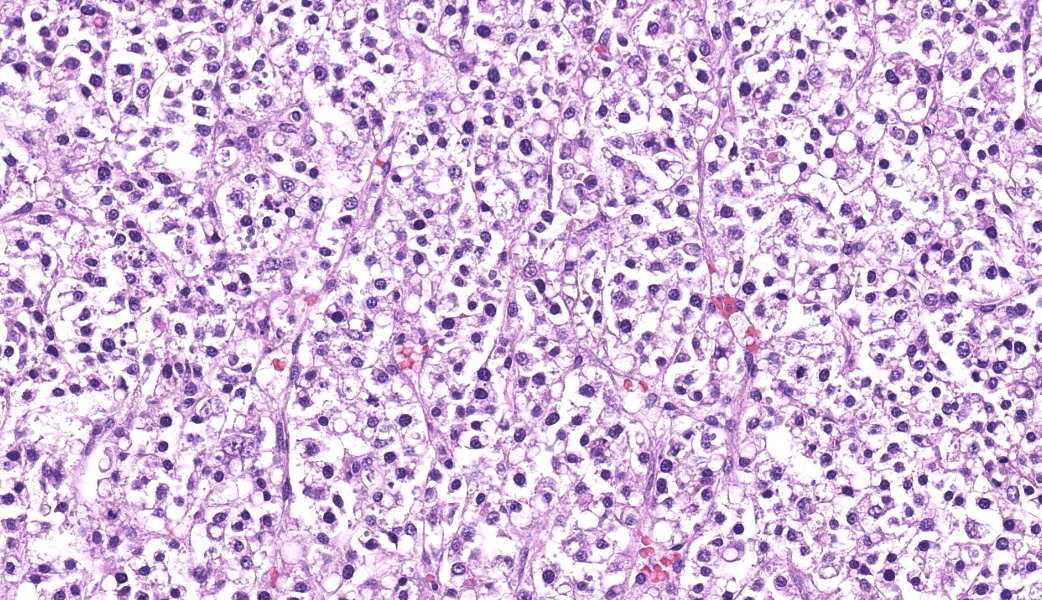
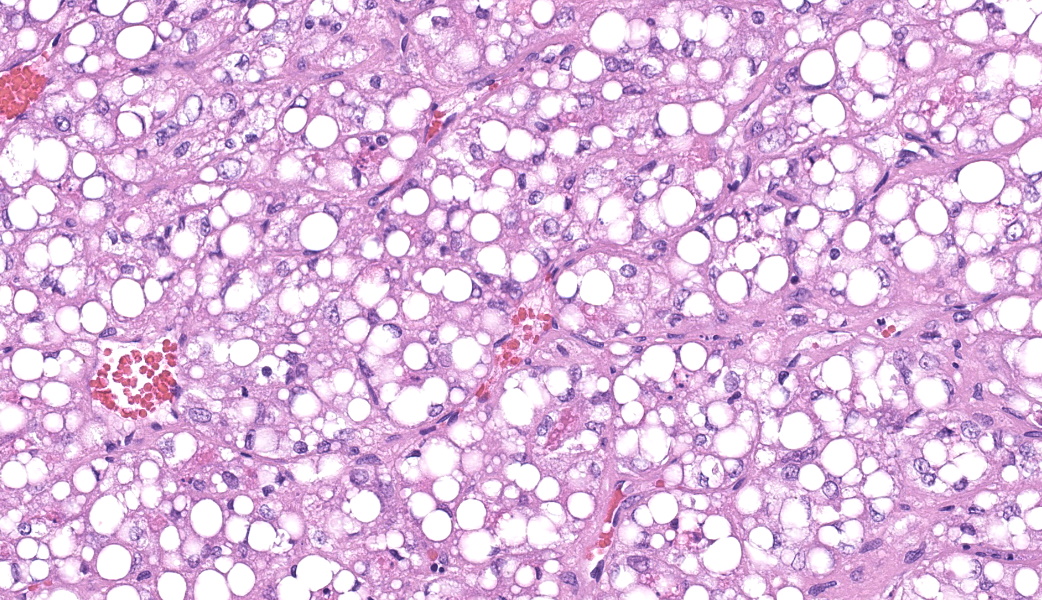
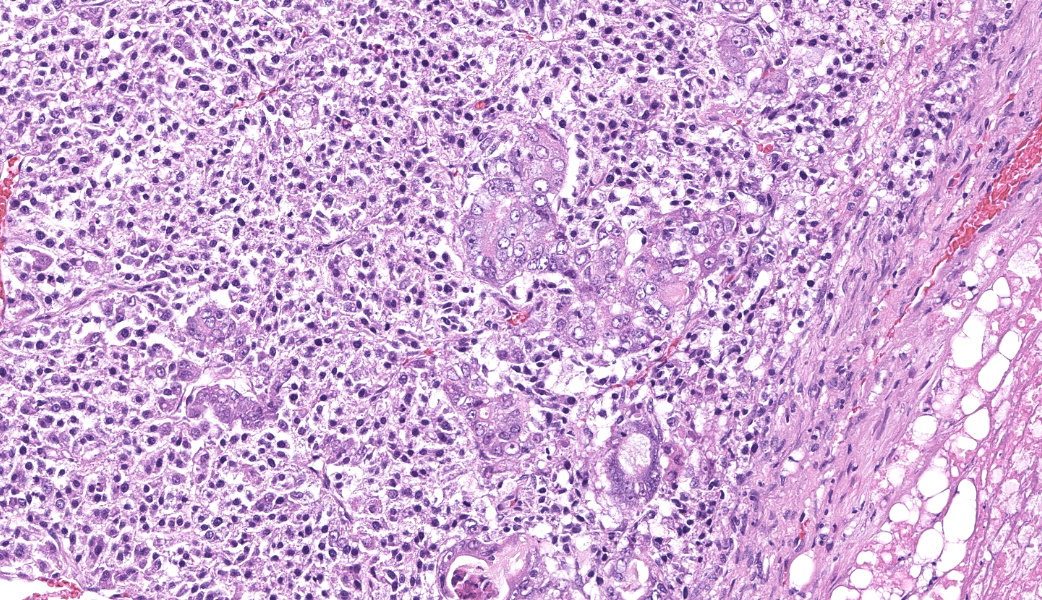
Captured in section is the optic chiasm, infundibulum, and pituitary. Effacing the pituitary and extending dorsally within hypothalamus, invading the surrounding leptomeninges, and infiltrating the piriform lobe is a poorly circumscribed, expansile and variably invasive, densely cellular neoplasm subdivided in lobules and packets by fibrovascular stroma. There are three neoplastic cell populations that haphazardly intermix, forming the mass effect. The predominate cell type (80%) consists of small, poorly differentiated polygonal cells with scant granular eosinophilic cytoplasm, indistinct cellular borders, and round nuclei with coarse chromatin arranged in nests and packets. Anisocytosis and anisokaryosis are mild with 17 mitotic figures per 10HPF (2.37mm2). The second cellular population is comprised of round to polygonal cells with indistinct cellular borders, scarce eosinophilic cytoplasm with prominent clear cytoplasmic vacuoles arranged in nests and packets. Nuclei are round to ovoid, eccentrically placed with finely stippled chromatin and prominent nucleolus. Anisocytosis and anisokaryosis are mild to moderate with rare mitotic figures identified. Finally, the third population are clusters of columnar cells with abundant amphophilic cytoplasm and indistinct cellular borders occasionally arranged in acini scattered throughout the mass. Nuclei are centrally placed, ovoid with finely stippled to vesicular chromatin. Anisocytosis and anisokaryosis are moderate with few scattered mitotic figures. Acini structures occasionally encircle granular basophilic to amphophilic material which sometimes has cellular debris. Throughout the neoplasm there are large regions of necrosis characterized by loss of tinctorial cellular staining, infiltrating viable and degenerate neutrophils, karyorrhectic debris, as well as hemorrhage and fibrin. Hemorrhage and neoplastic cells extend within the adjacent neuropil which exhibits spongy change. Multiple vessels are moderately to markedly ectatic and variably occluded by poorly organized fibrin and sometimes erythrocytes, platelets, and circulating leukocytes (thrombi). A few blood vessels are lined by hypertrophied endothelial cells and surrounded by cuffs of lymphocytes and plasma cells. There is rarefaction adjacent to the third ventricle as well as infiltration of Gitter cells.
Contributor's Morphologic Diagnosis:
Cerebrum: Malignant mixed germ cell tumor - suspect suprasellar germ cell tumor.
Contributor's Comment:
Masses in the pituitary and sellar region include primary pituitary neoplasia (e.g., adenoma or carcinoma), metastatic neoplasia (e.g., lymphoma, melanoma, mammary adenocarcinoma), meningioma, craniopharyngioma, and suprasellar germ cell tumor.1,5,8,13,15 In this case, the absence of systemic disease lowered the likelihood of primary pituitary or metastatic neoplasms. Histopathologic examination further excluded these differentials, revealing neoplastic cells with varied morphology - predominantly poorly differentiated germ cells, along with hepatoid and epithelial components. Based on the location, mixed neoplastic morphology, as well as marked local invasion and destruction, a diagnosis of suprasellar germ cell tumor was made.Mixed germ cell tumors are rare in domestic species, most frequently occurring in the gonads.4,13,16Extragonadal germ cell tumors are thought to arise from ectopic embryonic germ cells that become widely distributed.1In dogs, extragonadal tumors have been commonly reported in the suprasellar region with isolated cases also reported in the spinal cord and eye.2,3,5,8,9,11,18 Key features of suprasellar germ cell tumors include: a midline mass effect above the sella turcica and dorsal to the pituitary gland; pleomorphic histomorphology with the tumor being composed of several distinct cell types including populations which resemble seminoma/dysgerminoma as well as secretory glandular and/or squamous elements (teratomatous differentiation); and positive immunoreactivity for alpha-fetoprotein (AFP).18 In this case, all three criteria for a suprasellar germ cell tumor could not be met as AFP immunohistochemistry was unavailable at the laboratory.
Given the overlapping location, another differential considered in this case was craniopharyngioma. These tumors are presumed to arise from remnants of Rathke's pouch and are histologically characterized by sheets of round to polygonal neoplastic cells and clumps of palisading epithelial cells supported on a collagenous stroma1,13 Distinguishing between craniopharyngioma and suprasellar germ cell tumors can be challenging, and differentiation often relies on the assessment of AFP immunoreactivity. AFP is produced by the yolk sac of a developing fetus and serves as a useful marker for germ cell tumors in both humans and dogs.10,18 Neoplastic cells of suprasellar germ cell tumors exhibit AFP immunoreactivity, whereas craniopharyngiomas lack such reactivity. Further complicating differentiation between these neoplasms, the diagnosis of a suprasellar germ cell tumor is not precluded with weak or absent AFP immunoreactivity.2
Clinical signs associated with tumors in the pituitary region often include altered pituitary hormone secretion (e.g., hyperadrenocorticism) and can progress to deficits in cranial nerve function as well as central nervous system dysfunction caused due to tumor extension.15 In the present case, clinicopathologic data were unavailable, and there was no history of underlying endocrinopathy. The intensifying cranial nerve deficits and declining mentation were attributed to the tumor's expansive growth and broad regions of necrosis.
Contributing Institution:
National Institutes of Health Comparative Biomedical Scientist Training Program (CBSTP) in collaboration with Colorado State University Veterinary Diagnostic Laboratory
www.nih-cbstp.nci.nih.gov
www.vetmedbiosci.colostate.edu/vdl/
JPC Morphologic Diagnosis:
Cerebrum, thalamus: Suprasellar germ cell tumor.
JPC Comment:
This final case provided an excellent opportunity for discussion of the complexities of midline embryologic tumors and for a brief review of cranial nerve anatomy. This helped participants understand how a midline suprasellar mass might disrupt multiple cranial nerve pathways either through direct compression, distortion of the diencephalon, or secondary effects on the brainstem.
Anatomic orientation was, as with all four of these cases, the next challenge. This cerebral section included thalamus with optic chiasm, third ventricle, and paleocortex, placing this tumor squarely in the suprasellar region. As mentioned by the contributor, the most common locations for extragonadal germ cell tumors in dogs include the suprasellar region, mediastinum, eye, and spinal cord.10 They are often seen in young to middle-aged dogs, sometimes causing neurological or visual deficits.10
Immunohistochemistry plays a central role in the diagnosis. Participants were cautioned that pancytokeratin can cross react with GFAP, a pitfall that can mislead pathologists when evaluating tumors of the CNS.7 In this case, the neoplasm exhibited weak to moderate immunoreactivity for alpha-fetoprotein (AFP), supporting germ cell differentiation.
The differential diagnoses discussed in this case included craniopharyngioma, teratoma, and pituitary carcinoma, all of which can arise in or near the sella turcica. However, the combination of midline location, mixed cellular morphology, and AFP immunoreactivity align best with a mixed germ cell tumor under the 2021 WHO classification guidelines. Among the listed suprasellar neoplasms, this was the diagnosis that participants agreed best fit the morphologic and immunophenotypic profile.
Dr. Koehler also emphasized the developmental significance of the midline. This region is a crossroads of embryologic migration, fusion, and differentiation, making it a hotspot for tumors derived from ectopic germ cells. The presence of multiple divergent cell populations within the tumor further supported this developmental origin.
Finally, the group discussed the contributor's use of the term "malignant." Some participants preferred not to use that term, noting that primary brain tumors can be fatal due to location alone, even when their biological behavior is histologically benign. While this neoplasm did show histologic invasion and necrosis, there is no established prognostic literature for canine suprasellar germ cell tumors and applying the term "malignant" risks implying a known clinical course. Dr. Koehler framed this as a bit of a philosophical issue for the intents and purposes of conference, however, because, in neuro-oncology, "malignancy" is often a function of where a tumor is, not just what it is.12
References:
- Cantile C., Youssef S. Nervous System. In: Jubb, Kennedy, and Palmer's Pathology of Domestic Animals, ed. Maxie M.G. 6th edition. Philadelphia, USA: Elsevier, vol 1, p403-404.
- Cook L, Tensley M, Drost WT, et. al. MRI findings of suprasellar germ cell tumors in two dogs.J Am Animal Hosp Assoc. 2018;54(3):167-172.
- Ferreira AJ, Peleteiro MC, Carvalho T, Correia JM, Schulman FY, Summers BA. Mixed germ cell tumour of the spinal cord in a young dog. J Small Anim Pract. 2003;44(2):81-84.
- Foster RA. Male Genital System. In: Jubb, Kennedy, and Palmer's Pathology of Domestic Animals, ed. Maxie M.G. 6th edition. Philadelphia, USA: Elsevier, vol 3:495-496.
- Hare WR. Primary suprasellar germ cell tumor in a dog. J Am Vet Med Assoc. 1993;203(10):1432-1433.
- Higgins RJ, Bollen AW, Dickinson RJ, Siso-Llonch S. Tumors of the Nervous System. In: Tumors in Domestic Animals, ed. Meuten DJ. 5th edition. Newark, USA: Wiley, p834-891.
- Kriho VK, Yang HY, Moskal JR, Skalli O. Keratin expression in astrocytomas: an immunofluorescent and biochemical reassessment. Virchows Arch. 1997;431(2):139-47.
- Miller MA, Bruyette DS, Scott-Moncrieff JC, et al. Histopathologic Findings in Canine Pituitary Glands. Vet Pathol. 2018;55(6):871-879.
- Nyska A, Harmelin A, Baneth G, et al. Suprasellar differentiated germ cell tumor in a male dog. J Vet Diagn Invest. 1993;5(3):462-467.
- Patterson-Kane JC, Schulman FY, Santiago N, McKinney L, Davis CJ. Mixed germ cell tumor in the eye of a dog. Vet Pathol. 2001;38(6):712-714.
- Rech RR, Souza SF, Silva MC. et al. Suprasellar germ cell tumor in a dog.Ciência rural.2008;38(3):830-832.
- Rees JH. Diagnosis and treatment in neuro-oncology: an oncological perspective.Br J Radiol. 2011;84 Spec No 2(Spec Iss 2):S82-S89.
- Rissi DR. A retrospective study of skull base neoplasia in 42 dogs. Vet Diagn Invest. 2015;27(6):743-748.
- Robinson NA, Manivel JC, Olson EJ. Ovarian mixed germ cell tumor with yolk sac and teratomatous components in a dog. Vet Diagn Invest. 2013;25(3):447-452.
- Rosol TJ, Gröne A. Endocrine Glands. In: Jubb, Kennedy, and Palmer's Pathology of Domestic Animals, ed. Maxie M.G. 6th edition. Philadelphia, USA: Elsevier, vol 3, p287-288.
- Rosol TJ, Meuten DJ. Tumors of the Endocrine Glands. In: Tumors in Domestic Animals, ed. Meuten DJ. 5th edition. Newark, USA: Wiley, p766-833.
- Schlafer DH, Foster RA. Female Genital System. In: Jubb, Kennedy, and Palmer's Pathology of Domestic Animals, ed. Maxie M.G. 6th edition. Philadelphia, USA: Elsevier, vol 3, p377-378.
- Valentine BA, Summers BA, de Lahunta A, White CL 3rd, Kuhajda FP. Suprasellar germ cell tumors in the dog: a report of five cases and review of the literature.Acta Neuropathol.1988;76(1):94-100.