Signalment:
3-year-old, female bloodhound dog (
Canis familiaris).The dog was caught in the countryside and no history was available.
Gross Description:
Not reported.
Histopathologic Description:
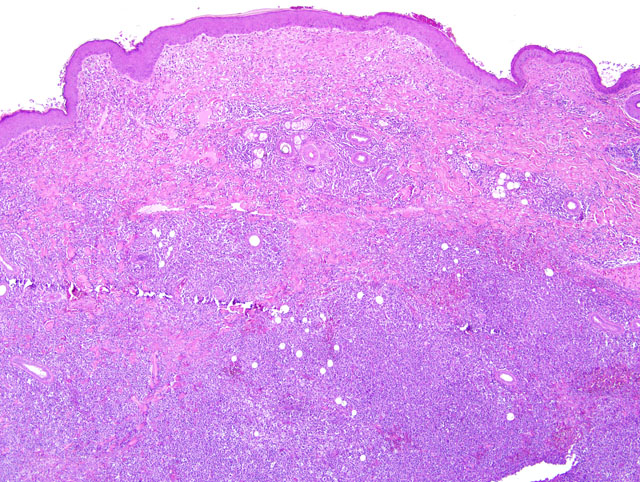
Haired skin and subcutis, posterior limb. Within the dermis and the hypodermis
there is a nodular (approximately 1.5 cm), slightly exophytic, infiltrative, poorly demarcated, unencapsulated,
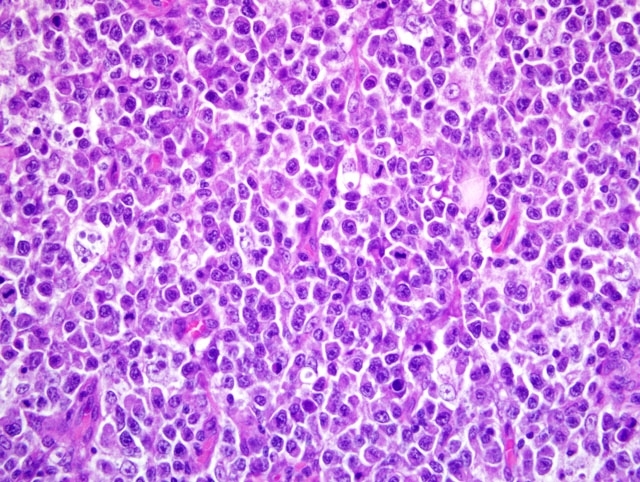
densely cellular lesion that effaces the dermal collagen and displaces the adnexa. The population is predominantly
composed by atypical discrete round cells with generally distinct cell borders and a small to moderate amount of
eosinophilic cytoplasm. Nuclei (approximately 1.5-2 x RBC) are central irregularly round and occasionally
indented, with finely stippled chromatin, and one generally indistinct nucleolus. Mitoses average 5 per high power
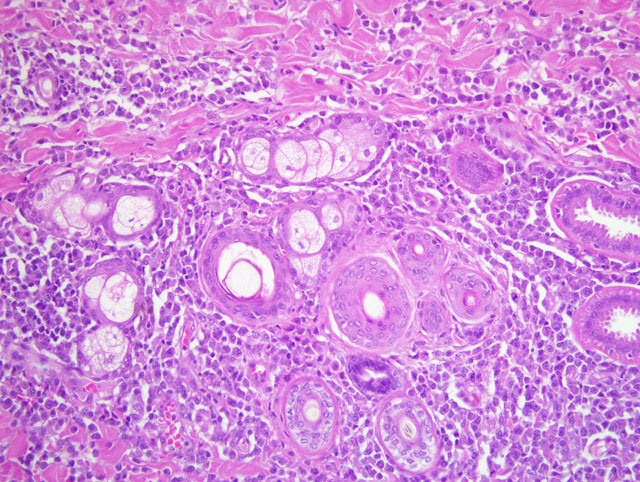
field. The atypical cells show occasional epidermal and follicular epitheliotropism. In association there is a second
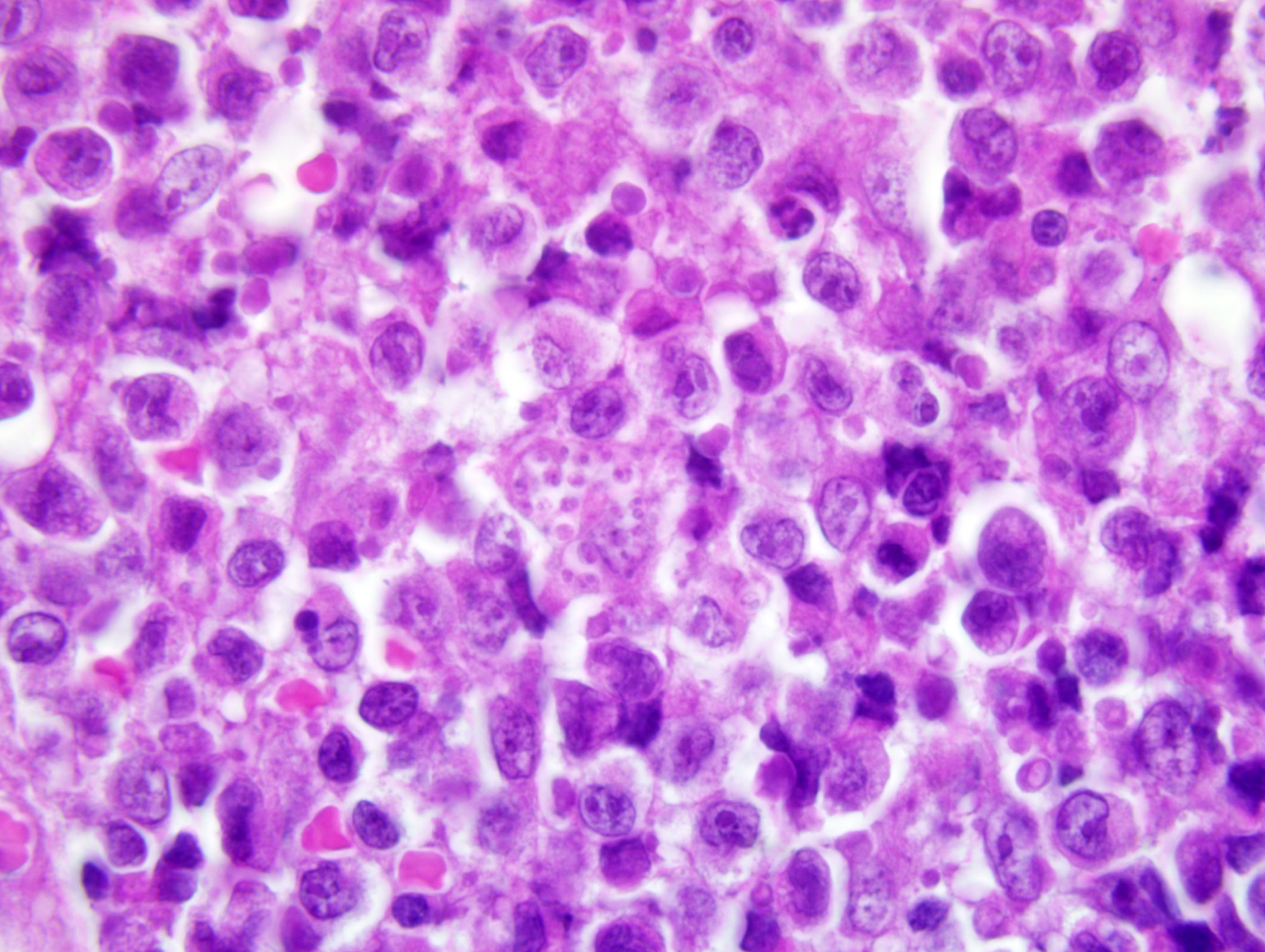
cellular population composed of high numbers of disseminated protozoa-laden macrophages. Intrahistiocytic
protozoal amastigotes are evident; they are 2-3 um in diameter with clear cytoplasmic halo, basophilic nucleus, and
a smaller adjacent (perpendicular) kinetoplast (consistent with
Leishmania spp. amastigotes). In addition, numerous
plasma cells and Mott cells and occasional small lymphocytes are also disseminated within and around the lesion,
and multifocally extend into the subcutis where they are predominantly focused around blood vessels. There is also
multifocal ulceration associated with degenerate and non-degenerate neutrophils, necrotic debris, and collagen lysis.
There is diffuse parakeratotic hyperkeratosis. The superficial dermis is multifocally mildly expanded by edema and
ectatic lymphatics.
Immunohistochemistry for CD3, CD5, CD79a, CD20 was performed (not submitted). The predominant atypical
population showed a moderate diffuse cytoplasmic staining for CD3. Staining for CD5, CD20, and CD79a was
negative. A nonspecific nuclear staining was detected for CD79a.
Morphologic Diagnosis:
Haired skin and subcutis, posterior limb: Epitheliotropic lymphoma
associated with histiocytic and lymphoplasmacytic dermatitis, severe, diffuse with myriad intrahistiocytic protozoal
amastigotes, consistent with
Leishmania spp.,
Canis familiaris, dog.
Condition:
Epitheliotropic lymphoma; Leishmania sp.
Contributor Comment:
Canine leishmaniasis (CL) is a systemic disease caused by different species of the genus
Leishmania that is transmitted by blood sucking phlebotomine sandflies. The majority of affected dogs present with
poor body condition, immunosuppression, lymphadenomegaly and excessive skin scaling. The disease is endemic
in the Mediterranean area. In the dog, the cellular immune response against
Leishmania is still not well defined,
although in affected individuals capable of overcoming the disease characteristic immune responses of type Th1
have been shown. Cutaneous epitheliotropic T-cell lymphoma in the dog is a rare neoplastic condition with
unknown etiology. In dogs, epitheliotropic T-cell lymphoma pursues a progressive course of disease with several
months to 2 years before death. The neoplastic population is characterized by infiltration of neoplastic T
lymphocytes with a specific tropism for the epidermis and the adnexal structures.(2)
From literature, prolonged antigenic stimulation and chronic immunosuppression plays a crucial role in the
etiopathogenesis of T-cell lymphoma.(1) Persistent environmental antigens act as a stimulus for chronic T-cell
activation and proliferation and progression to a clonal expansion has been suggested as a possible cause of
epitheliotropic lymphoma in humans.(3) To our knowledge some reports are present describing association between
skin lymphoma and atopic dermatitis or chronic skin allergic disease. Our dog could further confirm that chronic
antigen stimulation may be an initiator of a clonal neoplastic T-cell population in the skin. Canine epitheliotropic
lymphoma has been further subtyped as a tumor predominantly of CD8-γδ-T cells. In the present case, a deeper
investigation of the immunophenotype was not possible since monoclonal antibodies available for detection of CD4
and CD8 on formalin fixed tissue biopsies were not available. The cell population appeared to be CD3+ and
therefore compatible with T-cell lymphoma.
JPC Diagnosis:
1. Haired skin and subcutis: Lymphoma.
2. Haired skin and subcutis: Dermatitis, histiocytic and lymphoplasmacytic, diffuse, moderate, with focal ulceration
and numerous intrahistiocytic protozoal amastigotes.
Conference Comment:
While conference participants agreed with the histologic diagnosis of malignant
lymphoma, neoplastic epitheliotropism was not observed in the slides examined during conference, suggesting this
is a case of cutaneous nonepitheliotropic lymphoma. The majority of cutaneous nonepitheliotropic lymphomas in
dogs and cats are of T-cell origin. Additionally, cutaneous lymphoma is more commonly epitheliotropic in dogs and
nonepitheliotropic in cats.(4)
Leishmania sp. have several adaptations that allow their entry into and survival within macrophages.(5)
- Lipophosphoglycans bind to C3b and iC3b and enhance phagocytosis, and protect organisms by scavenging
oxygen free radicals and inhibiting lysosomal enzymes.
- Gp63, a zinc-dependent proteinase, cleaves complement and some lysosomal antimicrobial enzymes.
- Proton-transporting ATPase allows the amastigotes to survive in the phagolysosomes extremely acidic
environment.
References:
1. Boutros N, Hawkins D, Nelson M, Lampert IA, Naresh KN: Burkitt lymphoma and leishmaniasis in the same
tissue sample in an AIDS patient. Histopathology
48:880-881, 2006
2. Fakhar M, Asgari Q, Motazedian MH, Monabati A: Mediterranean visceral leishmaniasis associated with acute
lymphoblastic leukemia (ALL). Parasitol Res
103:473-475, 2008
3. Foglia Manzillo V, Pagano A, Guglielmino R, Gradoni L, Restucci B: Extranodal γδ-T-cell lymphoma in a dog
with leishmaniasis. Vet Clin Pathol
37:298-301, 2008
4. Gross TL, Ihrke PJ, Walder EJ, Affolter VK: Skin Diseases of the Dog and Cat: Clinical and Histopathologic
Diagnosis, 2nd ed., pp. 882-883. Blackwell Publishing, Ames, IA, 2005
5. McAdam AJ, Sharpe AH: Infectious Diseases.Â
In: Pathological Basis of Disease, eds. Kumar V, Abbas AK,
Fausto N, Aster JC, 8th ed., pp. 388-390. Saunders Elsevier, Philadelphia, PA, 2010