Signalment:
8-year-old, female spayed Jack Russell mix (
Canis familiars).The referring veterinarian described pustule formation progressing to ulceration in the axillary and inguinal regions, ventral abdomen and around the vulva.
Gross Description:
NA
Histopathologic Description:
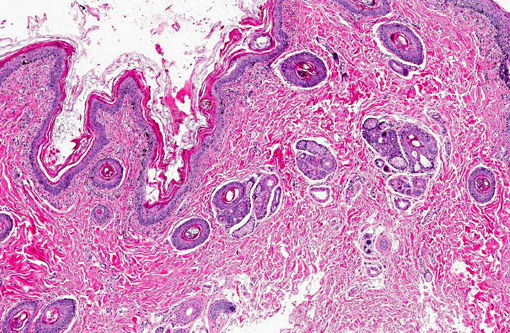
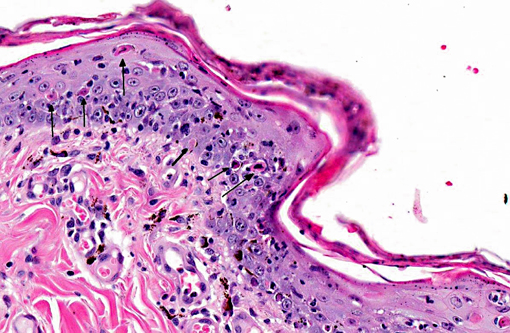
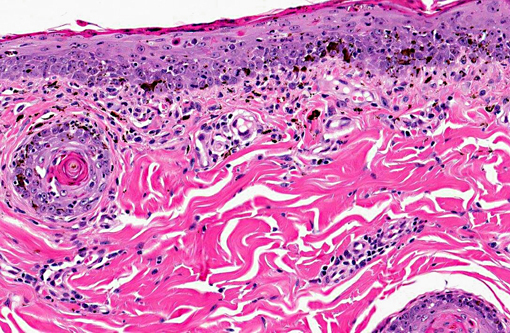
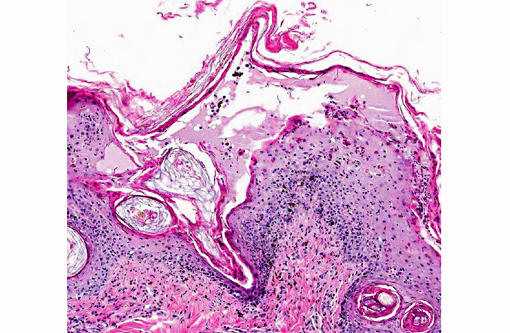
Haired skin: There are multiple focal plaque-like lesions alternating with small areas of normal skin. The epidermis is characterized by mild parakeratosis that often spans several hair follicles. The epidermis has mild to moderate thickening with apoptotic cells present in high numbers in all levels. Some of the apoptotic cells are surrounded by lymphocytes (satellitosis). Numerous intraepithelial or exocytosing lymphocytes are present. There is vacuolation along the basal layer with moderate pigmentary incontinence. These changes extend into the infundibular portion of the hair follicle sheaths. A mild diffuse interface and perivascular infiltrate of lymphocytes, plasma cells and histiocytes is present. Several hair follicles are in growth arrest and contain keratin plugs. Sebaceous glands are small and absent from a few follicles. In the area of the isthmus of the follicles with small or absent sebaceous glands, there is pyogranulomatous inflammation and vacuolation. Apocrine glands are mildly dilated. No fungal organisms are detected in routinely stained sections. A small colony of bacteria is associated with hair in the ostia of a single follicle. Rare coccoid bacteria are noted in the surface keratin debris.Â
Morphologic Diagnosis:
Haired skin: Dermatitis, interface, subacute, multifocal, moderate with apoptosis, mild parakeratotic hyperkeratosis, folliculitis and adnexal destruction (sebaceous gland)
Condition:
Erythema multiforme
Contributor Comment:
The clinical history, lesion distribution and histologic lesions are consistent with erythema multiforme (EM). The two major differential diagnoses for immune-mediated skin disease with interface dermatitis and apoptosis are erythema multiforme (EM) and all forms of lupus erythematosus (LE). The apoptosis observed in LE tends to be limited to the basal cell layer where vacuolation also occurs. The classic lesion in EM is apoptosis involving any cellular layer of the epidermis along with lymphocyte satellitosis.(4) There are usually aggregates of lymphocytes and histiocytes along the dermal-epidermal junction. Vacuolation and apoptosis of the basal cell layer occur, and there is variable pigmentary incontinence. Areas of ulceration are typically associated with additional infiltrates of neutrophils, eosinophils and plasma cells.Â
Erythema multiforme is a relatively uncommon skin disease reported in dogs, cats, horses and cattle that has been associated with a number of different triggers.(2,3) The pathogenesis of EM is not completely understood; however, this disease is thought to be a T-cell-mediated hypersensitivity reaction against a variety of antigens including drugs, viruses, bacteria and food substances.(1,3,5-9) EM has also been described as a paraneoplastic condition associated with a variety of tumor types.(1,4,10)
The most commonly incriminated drugs include trimethoprim-potentiated sulfonamides, penicillins and cephalosporins.(4,7,8) The dog in this case was medicated with trimethoprim-sulfa for cystitis prior to the onset of the cutaneous lesions.Â
Clinically, dogs present with an acute onset of erythematous annular macules, elevated circular plaques and papules that are most commonly involve the glabrous skin of the inguinal and axillary regions.(4) Mucocutaneous junctions, oral mucosa, ears and paw pads are also commonly affected. Two classifications for EM have been adopted from human nomenclature. EM minor includes patients with no more than one mucosal surface affected and <10% of the body surface affected. EM major is used for cases in which more than one mucosal surface and between 10% to 50% of the body surface is affected. A third syndrome, Stevens-Johnson syndrome, is reserved for patients with >50% of the body surface affected.Â
JPC Diagnosis:
Haired skin: Apoptosis, transepidermal, epidermal and follicular, multifocal, with necrosis, hydropic degeneration, subepidermal clefting, orthokeratotic hyperkeratosis, and neutrophilic and lymphohistiocytic interface dermatitis.
Conference Comment:
As the contributor notes in the above informative summary, EM is thought to be a T-cell mediated hypersensitivity in which the hosts cellular immune response is directed against keratinocyte-associated antigens. Such reactions have been reported to be associated with certain drugs, bacterial infections (staphylococcal folliculitis, pseudomonal otitis externa), food products, and epitheliotropic viral infections. In particular, conference participants discussed the association between EM and canine parvovirus type 2b (CPV-2b). There have been a few cases of EM reported in dogs associated with CPV-2b infection, including in a 2-month-old Great Dane puppy and, more recently, a litter of English Setter puppies.(2,6) It has been suggested that infection of stem cells and transient amplifying keratinocytes occurs following hematogenous dissemination of CPV-2b, thus leading to initiation of EM. The recent report suggests that, along with the multiple other possible initiating factors, CPV-2b should be considered as a potential initiator of EM in dogs.(6)
References:
1. Elmore S, Basseches J, Anhalt GJ, Cullen JM, Olivry T. Paraneoplastic pemphigus in a dog with splenic sarcoma.Â
Vet Pathol. 2005;42:88-91.
2. Favrot C, Olivry T, Dunston SM, et al. Parvovirus infection of keratinocytes as a cause of canine erythema multiforme.Â
Vet Pathol. 2000;37:647649.
3. Ginn PE, Mansell JEKL, Rakich PM. The skin and appendages. In: Maxie MG, ed.Â
Jubb, Kennedy and Palmers Pathology of Domestic Animals. 5th ed. Vol. 1. New York, NY: Elsevier Saunders; 2007:656.
4. Gross TL, Ihrke PJ, Walder EM, Affolter VK. Interface diseases of dermal-epidermal junction. In:
Skin Disease of Dogs and Cats: Clinical and Histopathologic Diagnosis. 2nd ed. Oxford, UK: Blackwell Science Ltd; 2005:52-68.
5. Itoh T, Nibe K, Kojimoto A, Mikawa M, Mikawa K, Uchida K, et al. Erythema multiforme possibly triggered by food substances in a dog.
J Vet Med Sci. 2006;68(8):869-871.
6. Woldemeskel M, Liggett A, Ilha M, Saliki JT, Johnson LP. Canine parvovirus-2bassociated erythema multiforme in a litter of English Setter dogs.Â
J Vet Diagn Invest. 2011;23:576-580.
7. Nuttall TJ, Malham T. Successful intravenous human immunoglobulin treatment of drug-induced Stevens-Johnson syndrome in a dog.Â
J Small Anim Pract. 2004;45:357-361.
8. Scott DW, Miller WH, Griffin CE. Immune mediated disorders, erythema multiforme. In:
Muller and Kirks Small Animal Dermatology. 6th ed. Philadelphia, PA: Saunders; 2001:729-740.
9. Scott DW. Erythema multiforme in a dog caused by a commercial nutraceutical product.Â
J Vet Clin Sci. 2008;1:1621.
10. Scott DW, Miller WH. Erythema multiforme in dogs and cats: Literature review and case material from the Cornell University College of Veterinary Medicine (198896).Â
Vet Dermatol. 1999;10:297309.
11. Tepper L, Spiegel IB, Davis GJ. Diagnosis of erythema multiforme associated with thymoma in a dog and treated with thymectomy.
J Amer Anim Hosp Assoc. 2011;47:e19-e25.