Signalment:
Gross Description:
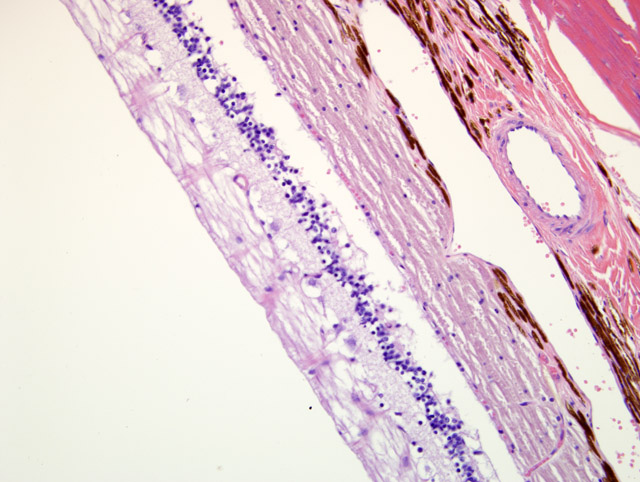
Histopathologic Description:
Morphologic Diagnosis:
Condition:
Contributor Comment:
A differential diagnosis for outer retinal degeneration/atrophy in a cat includes enrofloxacin toxicity, taurine deficiency, inherited retinal atrophy, and hypertensive retinopathy.
For an excellent summary of the events associated with the appearance of enrofloxacin retinal toxicosis in the cat, and the clinical, histopathologic, and ultrastructural ocular lesions associated with oral administration of enrofloxacin at 10 times the recommended dose in an experimental setting, readers are referred to reference 2. While the current recommended dosage of 5mg/kg/day seems to have substantially decreased cases of retinal toxicosis, the authors of the same reference conclude with the following statement: Investigation of the effects of administration of the recommended dosage of enrofloxacin on the retinas and CNS of cats is warranted.(2)
The exact mechanism of enrofloxacin retinal toxicosis is not known; however, any fluoroquinolone or structurally related compounds should be considered potentially retinotoxic in cats.(11) Risk factors predisposing cats to enrofloxacin retinal toxicosis include large doses or plasma concentration, rapid IV infusion of the antibiotic, prolonged courses of treatment, and age.(11) In cats, the combination of methylnitrosourea and ketamine hydrochloride induces retinal degeneration, but neither drug does so individually.(10)
The retinal lesion seen in taurine deficiency usually starts centrally, hence the disease name of feline central retinal degeneration, but can progress to diffuse retinal atrophy given enough time.(5,8) Due to taurine supplementation of commercial feline diets, the disease is fairly rare now, however, it has been induced by feeding dog food to cats.(1) Affected cats may also have dilated cardiomyopathy. If recognized early enough, both vision and cardiac function can be partially restored with appropriate dietary taurine levels.(4,7)
Inherited retinal atrophy, or progressive retinal atrophy, has been studied extensively in Abyssinians but has also been documented in Persians and speculated in several other cases.(3,6,9) In the Abyssinian there are two forms termed rod-cone dysplasia (autosomal dominant inheritance) and rod-cone degeneration (autosomal recessive inheritance), both of which may serve as an animal model of the human disease, retinitis pigmentosa.(6) Hypertensive retinopathy classically includes retinal detachment, subretinal effusion/hemorrhage and retinal and choroidal vessel medial hypertrophy and/or degenerative changes, none of which was seen in this case. Affected cats usually suffer from concomitant renal disease or hyperthyroidism. Renal histology was unremarkable. The thyroid glands (right thyroid enlarged at necropsy) were not examined histologically; however, the owner indicated the animal was given a thyroid medication (dosage unknown) suggesting this animal may have been treated for hyperthyroidism. If the hyperthyroidism was appropriately controlled the cat was likely normotensive although it may have experienced hypertension prior to treatment being initiated. If hyperthyroidism was insufficiently controlled the animal may have suffered from hypertension; however, as previously mentioned the eye lacks vascular changes consistent with chronic hypertension. Hyperthyroidism may have played a role in the myocardial lesion.
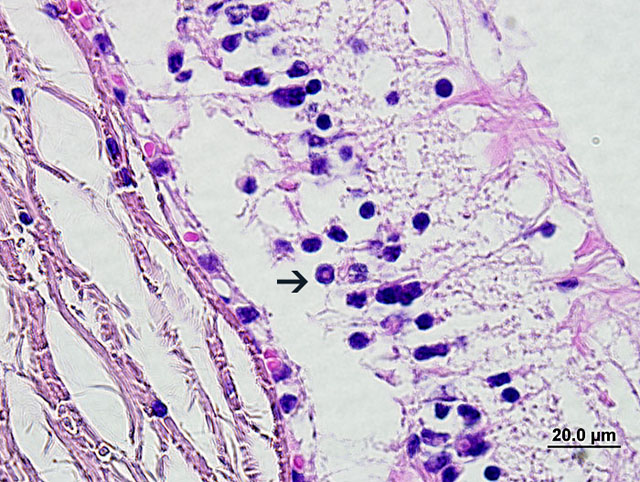
Causes and significance of the sporadic intranuclear inclusions (see images 1-4) are unknown. Potential artifact or nuclear membrane invaginations were considered. To the best of our knowledge, intranuclear inclusions of the inner nuclear layer in the cat are unreported
JPC Diagnosis:
Conference Comment:
Additionally, there was an active discussion during the conference regarding the few to moderate number of cells within the inner nuclear layer of the retina containing intranuclear, eosinophilic bodies. The consensus was that these bodies are cytoplasmic invaginations into the nuclei and should not be confused with viral inclusion bodies.
References:
2. Ford MM, Dubielzig RR, Giuliano EA, Moore CP, Narfstrom KL: Ocular and systemic manifestations after oral administration of a high dose of enrofloxacin in cats. Am J Vet Res 68:190-202, 2007
3. Glaze MB: Congenital and hereditary ocular abnormalities in cats. Clin Tech Small Anim Pract 20:74-82, 2005
4. Hayes KC, Rabin AR, Berson EL: An ultrastructural study of nutritionally induced and reversed retinal degeneration in cats. Am J Pathol 78:505-524, 1975
5. Leon A, Levick WR, Sarossy MG: Lesion topography and new histological features in feline taurine deficiency retinopathy. Exp Eye Res 61:731-741, 1995
6. Narfstrom K: Hereditary and congenital ocular disease in the cat. J Feline Med Surg 1:135-141, 1999
7. Pion PD, Kittleson MD, Rogers QR, Morris JG: Myocardial failure in cats associated with low plasma taurine: a reversible cardiomyopathy. Science 237:764-768, 1987
8. Rabin AR, Hayes KC, Berson EL: Cone and rod responses in nutritionally induced retinal degeneration in the cat. Invest Ophthalmol 12:694-704, 1973
9. Rah H, Maggs DJ, Blankenship TN, Narfstrom K, Lyons LA: Early-onset, autosomal recessive, progressive retinal atrophy in Persian cats. Invest Ophthalmol Vis Sci 46:1742-1747, 2005
10. Schaller JP, Wyman M, Weisbrode SE, Olsen RG: Induction of retinal degeneration in cats by methylnitrosourea and ketamine hydrochloride. Vet Pathol 18:239-247, 1981
11. Wiebe V, Hamilton P: Fluoroquinolone-induced retinal degeneration in cats. J Am Vet Med Assoc 221:1568- 1571, 2002
12. Young B, Lowe JS, Stevens A, Heath JW: Special sense organs. In: Wheater's Functional Histology, A Text and Color Atlas, ed. Young B, Lowe JS, Sevens A, Heath JW, 5th ed., pp. 400-413. Churchill Livingstone, Elsevier, Philadelphia, PA, 2006