CASE II:
Signalment:
Four-year-old Holstein cow (Bos taurus taurus).
History:
A 5-year-old Holstein cow was presented with a history of breathing difficulty, and progressive weight loss before calving. The cow was treated with tetracycline, dipyrone, and flunixin meglumine for approximately two weeks; however, the doses were not recorded by the farmer. After calving, weight loss worsened and muffled heart sounds were noticed 3 days before the animal died.
Gross Pathology:
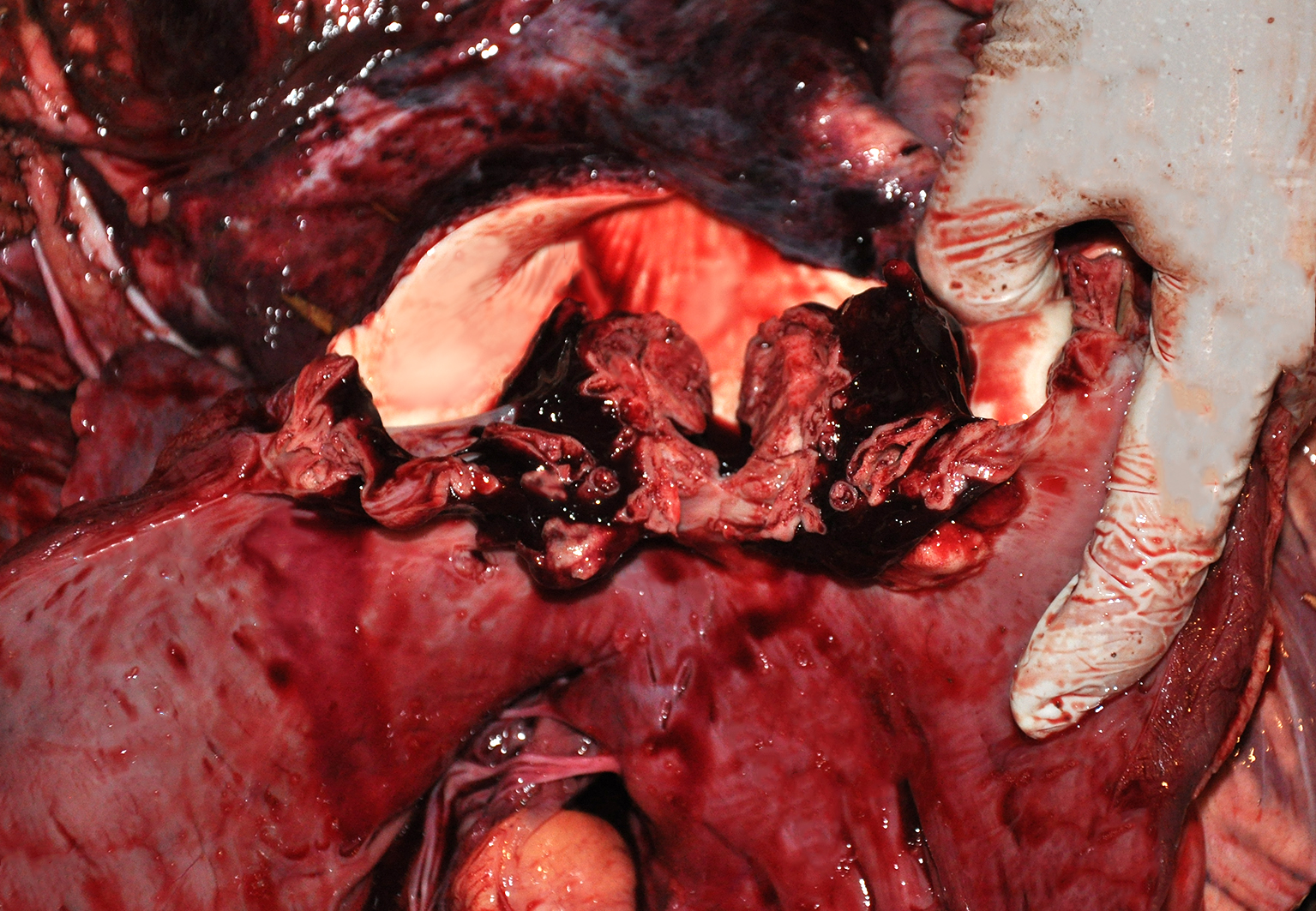
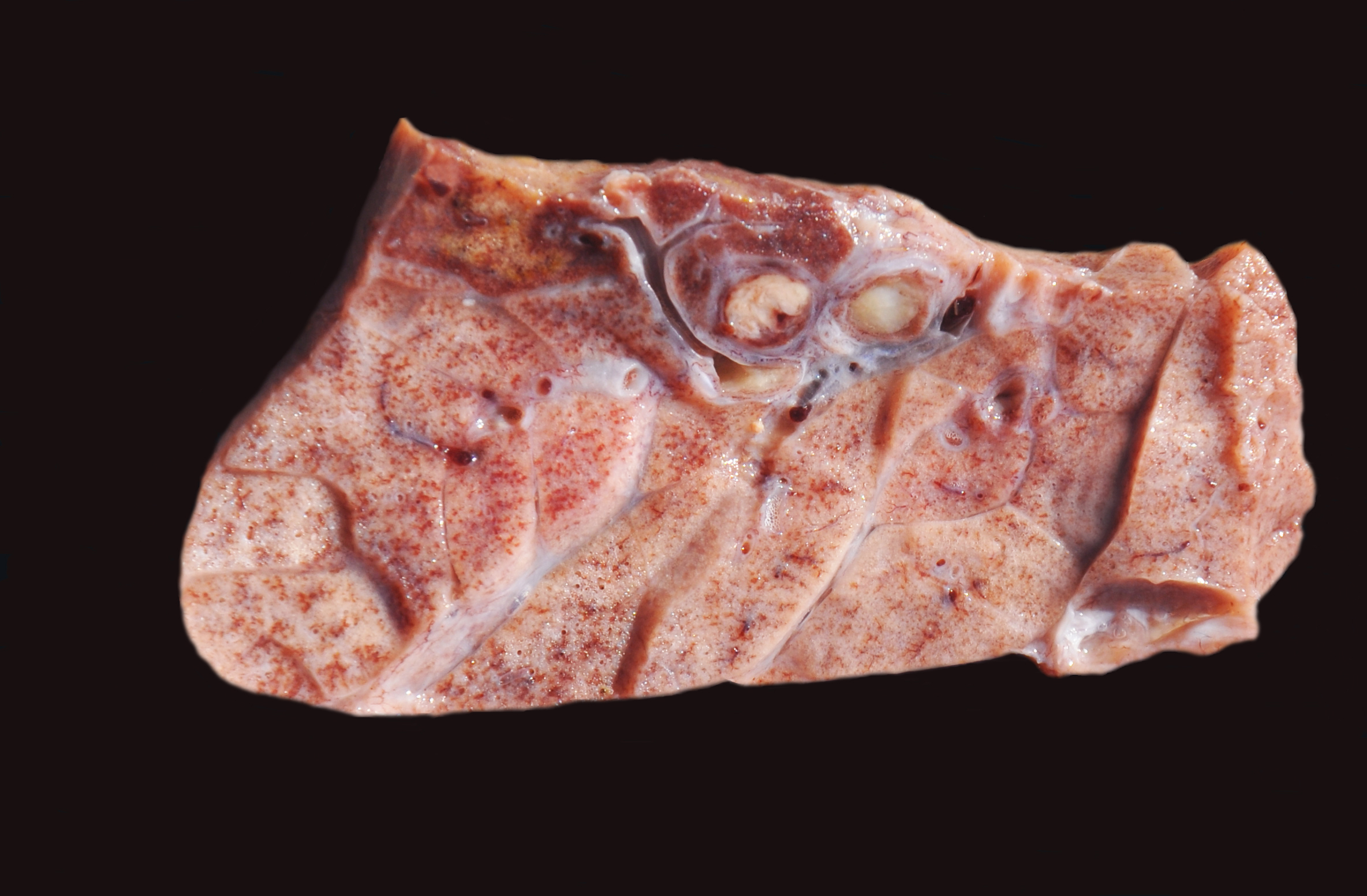
A five-year-old Holstein cow was submitted for necropsy examination presenting a poor body condition and markedly pale mucous membranes. Grossly, extensive areas of hemorrhage were observed in the pericardium, epicardium, extending to the pulmonary artery. Examination of the heart cavities demonstrated a friable, irregular, mottled white, brown and red vegetative mass of approximately 5.0 x 3.0 x 2.0 cm firmly adhered to all cusps of the pulmonary valve (Figure 1). In the lungs, multifocal to coalescent areas of consolidation were observed in all pulmonary lobes, and these were characterized by firm consistency, reddish color, and were associated with interlobular edema. Additionally, multiple yellowish, firm structures were observed occluding blood vessels (thrombi) (Figure 2). The abomasum was markedly distended and filled with free non coagulated blood, associated with severe multifocal mucosal ulcerations. Hemorrhagic content was seen throughout the intestinal tract. No other lesions were observed in the remaining organs.
Laboratory Results:
Refrigerated samples of the lungs and valve were cultured and submitted to the 16S
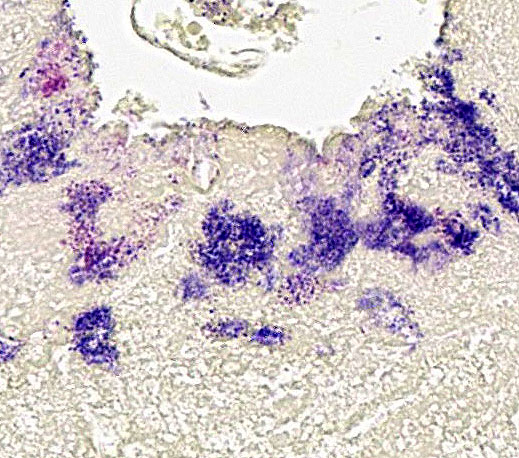
rRNA gene sequencing that revealed Helcococcus ovis in the valve sample. No bacterial growth was obtained from the lung sample. Gram stain was performed in the lungs and valve showing abundant Gram-positive coccoid bacterial aggregates inside arterioles in the lungs and in the vegetative structures in the heart.
Microscopic Description:
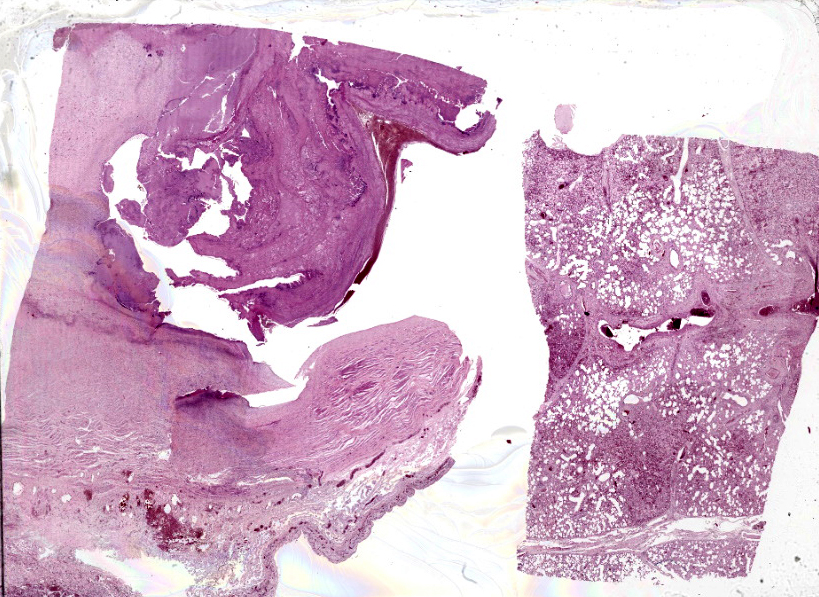
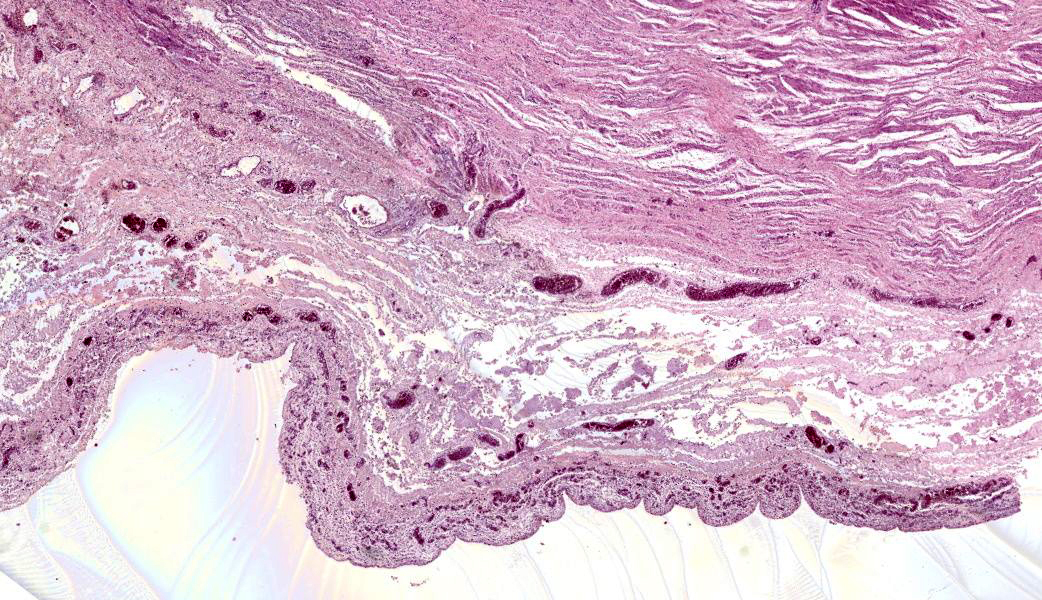
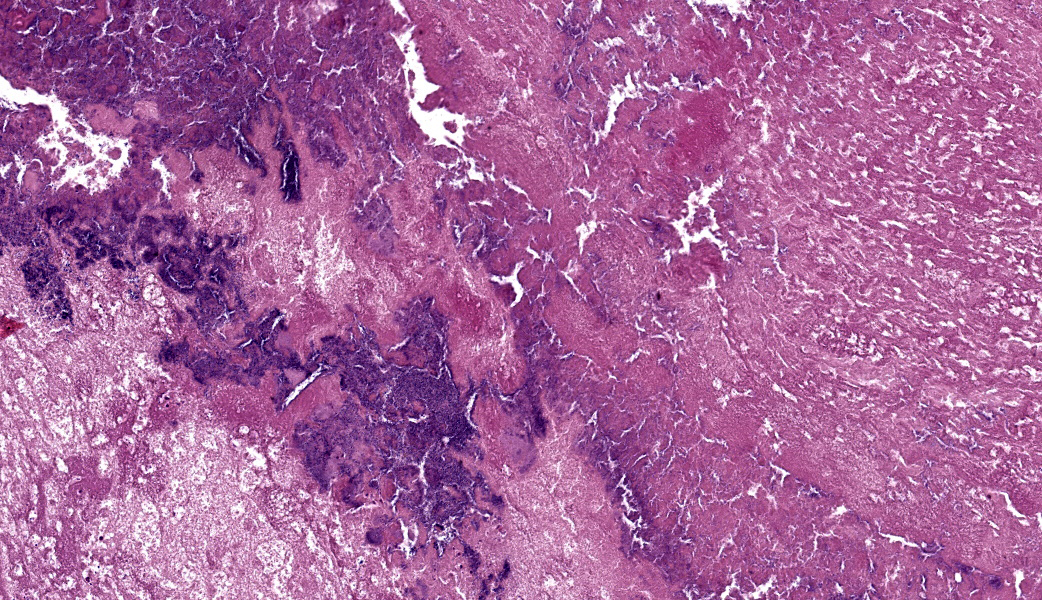
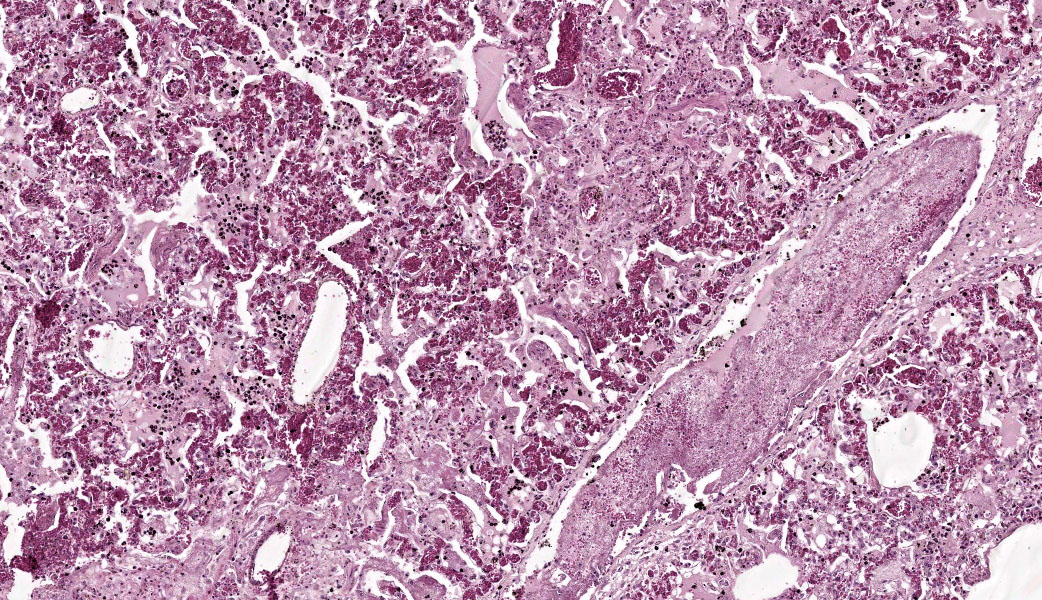
The submitted slides present one section of heart and one section of lung (Figure 3). In the heart, severe thickening of the pulmonary valve endocardium is observed, characterized by marked proliferation of fibrovascular tissue, inflammatory infiltrate of non-degenerate and degenerate neutrophils, as well as macrophages, deposition of eosinophilic material (fibrin), cellular debris, and an abundant number of coccoid basophilic bacterial colonies. The lung exhibits multifocal severe thrombosis characterized by large amounts of fibrin deposition inside large and small arterioles, associated with Gram-positive bacterial colonies (Figure 4), similar to those seen in the pulmonary valve (not all slides contain bacterial colonies in the lungs). Adjacent to these areas, in the alveolar space, a moderate inflammatory infiltrate of neutrophils, areas of necrosis, edema, and fibrosis, as well as free erythrocytes (hemorrhage), and a moderate number of macrophages are observed. Interlobular septa are thickened by fibrous connective tissue and inflammatory infiltrate of non-degenerate and degenerate neutrophils, as well as fibrin deposition. There is also a moderate thickening of the visceral pleura, characterized by the proliferation of fibrous connective tissue.
Contributor's Morphologic Diagnosis:
Heart: Valvulitis and Endocarditis, fibrinosuppurative, diffuse, severe, with intralesional coccoid bacterial aggregates.
Lung: Pneumonia, suppurative, thromboembolic, multifocal to coalescent, severe, with intralesional coccoid bacterial aggregates.
Contributor's Comment:
The gross and microscopic findings observed in this case were compatible with vegetative valvular endocarditis and thromboembolic pneumonia caused by a bacterial agent, that was confirmed through culture and molecular analysis as Helcococcus ovis. This bacterium is a gram-positive coccus that has been associated with multiple clinical presentations, such as mastitis in sheep, endocarditis and abortion in cattle, and pulmonary abscesses in horses.2,6 Reports in Germany suggest that H. ovis is an emerging pathogen that can lead to valvular endocarditis.5 Differential diagnoses must include other bacterial agents, such as Streptococcus sp. and Trueperella pyogenes, which are the most common agents associated to endocarditis in cattle.1 Besides bacteria, occasionally mycotic or parasitic infection can lead to endocarditis, as a result of systemic mycotic disease caused by zygomycetes or Aspergillus sp., or larvae of Strongylus vulgaris.7
Endocarditis is the inflammation of endocardium, and even though any part of this tissue layer may be affected, lesions usually affect primarily the valves.7 In cattle, the tricuspid valve, followed by the mitral valve are more commonly involved in endocarditis, and the pulmonary valve is considered to be an uncommon presentation.1,5 Usually, endocarditis in cattle is associated with traumatic lesions, followed by bacterial infection, with sustained or recurrent bacteremia, such as in cases of peritoneal abscesses, hepatic abscesses, mastitis and metritis.7 It is not well understood how H. ovis enters the bloodstream or its original habitat; however, Rothschild suggested that the possible source of infection could be the skin.8 Bacteria from the skin can enter into the systemic circulation due to lesions that break the skin barrier, leading to bacteremia, and may adhere to heart valves.7 In the present case, no surgical procedure was done, nor open wound or history of previous diseases, including mastitis or metritis, were observed or reported. Even though the cow presented abomasal ulcers at the time of necropsy, those were considered to be acute as a result of anti-inflammatory treatment and not related to the endocarditis.
Post reported a case of valvular endocarditis by H. ovis in the right atrioventricular valve of a bull in the state of North Carolina (USA), and the microscopic findings, such as severe inflammatory infiltrate and areas of necrosis, were similar to those observed in this case.6 Similar patterns of chronic endocarditis caused by H. ovis were described by Kutzer, which consisted of valvular emboli characterized by a luminal zone showing unorganized fibrinous exudate.5
Common clinical signs of endocarditis in cows are reported as progressive weight loss,
drop in milk production, lameness, tachycardia with auscultation of heart murmur, fever, and consequent respiratory distress.1,7 In the case here described, the owners noticed weight loss, milk drop and fever, however, these clinical signs were thought to be associated with other infectious diseases, including tick fever. Valvular endocarditis is usually fatal, and valvular damage and embolism are common sequelae.4,7 Some portions of the vegetative lesion can detach and be carried through the blood circulation as emboli and, in some cases such as the one described here, those emboli are also septic, carrying the bacterial agent involved in the endocarditis. Emboli that arise from the right heart usually produce pulmonary abscessation or pulmonary thrombosis, as observed in this case.7 The lung lesions were consistent with pulmonary thromboembolism due to the right heart endocarditis. Surrounding the thrombi areas in the lungs, areas of coagulative necrosis with inflammatory cells and hemorrhage could be observed.
In the case here described, it was only possible to culture the bacteria from the heart sample (affected valve), and not from the lungs. This difference may be caused by several features related to the location of bacterial aggregates, bacteria behavior, selection of sampling area and previous antibiotic treatment. One of the main characteristics of H.ovis is that it shows growth in satellites, and the lack of inoculation with other bacteria (e.g. Staphylococcus aureus) may have disadvantaged the isolation of the agent.5 The methods used in classical bacteriology are unable to reach the definitive diagnosis of infection by H.ovis, and molecular analysis is necessary to identify this bacterium.
Contributing Institution:
Setor de Patologia Veterinaria, Universidade Federal do Rio Grande do Sul, Brazil Faculdade de Veterinaria Universidade Federal do Rio Grande do Sul Setor de Patologia Veterinaria http://www.ufrgs.br/patologia
JPC Morphologic Diagnosis:Pulmonary valve: Valvulitis, fibrinosuppurative, chronic-active, focally extensive, severe, with remodeling and colonies of cocci.
Lung: Pneumonia, embolic, fibrinosuppurative, chronic-active, diffuse, severe with marked edema and septic thrombi.
JPC Comment:
This case challenged participants right from the start with tissue identification. Several attendees initially thought they were looking at the aorta or another large elastic artery. Only after it was revealed in conference to be heart valve did many realize the tissue in question was pulmonic valve. This tissue ID, which very few participants managed to get to before conference, could be aided by a small region of cardiac muscle (likely at the valve root, with central nuclei and fibrosis, a subtle but critical clue. This set the tone for a case that required attention to anatomic context and lesion distribution.
Once oriented, participants quickly recognized the hallmarks of valvular endocarditis with septic thromboembolic pneumonia, a classic pairing when emboli originate from the right heart. A separate case in a non-human primate was seen in this year's Conference 5, Case 2. Dr. Brown emphasized this point: right-sided endocarditis causes pulmonary emboli, whereas left-sided endocarditis produces systemic infarcts (especially in the kidneys). The lung lesions in this cow (fibrinosuppurative embolic pneumonia with septic thrombi) were textbook examples of this pathogenesis.
Differentials for bovine endocarditis were reviewed, with Streptococcus bovis and Trueperella pyogenes topping the differential list for many participants. These two bacteria remain the most common etiologies for this disease in cattle.1 However, the contributor identified the culprit as Helcococcus ovis. There is also a recently described related species that is able to cause human disease called Helcococcus bovis, which is closely related to H. ovis.3 This organism is becoming recognized as an emerging pathogen in ruminants, though it is still unfamiliar to many diagnosticians.3,4,5 Dr. Brown noted that Helcococcus ovis and H. bovis are believed to be part of the skin microbiome, gaining access to the bloodstream through minor breaches in the integument.5 H. ovis has also demonstrated widespread resistance to tetracyclines.3
A particularly interesting point mentioned in conference was the organism's growth behavior. Helcococcus bovis demonstrates satellite growth, requiring the presence of Staphylococcus spp. on blood agar to grow robustly.5 This helps to explain why the organism was isolated from the valve, where bacterial load was highest, but not from the lungs, despite clear histologic evidence of septic emboli. Dr. Brown reminded participants that failure to culture an organism does not exclude its presence, especially when dealing with fastidious bacteria.
This cow also had abomasal ulcers, which prompted a brief review of NSAID-associated ulceration. Dr. Brown walked participants through the mechanism: NSAIDs inhibit prostaglandin synthesis, which among other deleterious processes, leads to decreased bicarbonate secretion. A lack of bicarbonate results in increased abomasal acidity, leading to mucosal injury and ulcer formation. These lesions were considered acute and unrelated to the endocarditis by the contributor.
References:
- Buczinski S, Tsuka T, Tharwat M: The diagnostic criteria used in bovine bacterial endocarditis: A meta-analysis of 460 published cases from 1973 to 2011. Vet J. 2012;193(2):349-357.
- Colins MD, Falsen E, Foster G, Monasterio LR, Dominguez L, Fernandez-Garazabal JF: Helcococcus ovis sp. nov., a Gram-positive organism from sheep. Int J Syst Bacteriol. 1999;49(4):1429-1432.
- Cunha F, Zhai Y, Casaro S, et al. Pangenomic and biochemical analyses of Helcococcus ovisreveal widespread tetracycline resistance and a novel bacterial species, Helcococcus bovis. Front Microbiol. 2024;15:1456569.
- Kemper RT, Lopes BC, Rosa RB, et al: Valvular endocarditis associated with Helcococcus ovis in a cow in Southern Brazil. Cienc Rural. 2020. In press.
- Kutzer P, Schulze C, Engelhardt A, Wieler LH, Nordhoff M: Helcococcus ovis, an emerging pathogen in bovine valvular endocarditis. J Clin Microbiol. 2008;46(10):3291-3295.
- Post KW, Rushton SD, Billington SJ: Valvular endocarditis associated with Helcococcus ovis infection in a bovine. J Vet Diagn Invest. 2003;15(5):473-475.
- Robinson WF, Robinson NA. Cardiovascular system. In: MAXIE MG, ed. Pathology of Domestic Animals-Volume 3. 6th ed. St. Louis, USA: Elsevier; 2016:16-101.
- Rothschild CM, Oaks JL, Schaupp JK, Rurangirwa FR, Sellon DC, Hines MT: Helcococcus ovis isolated from a pulmonary abscess in a horse. J Clin Microbiol. 2004;42(5):2224-2226.