Signalment:
Gross Description:
Histopathologic Description:
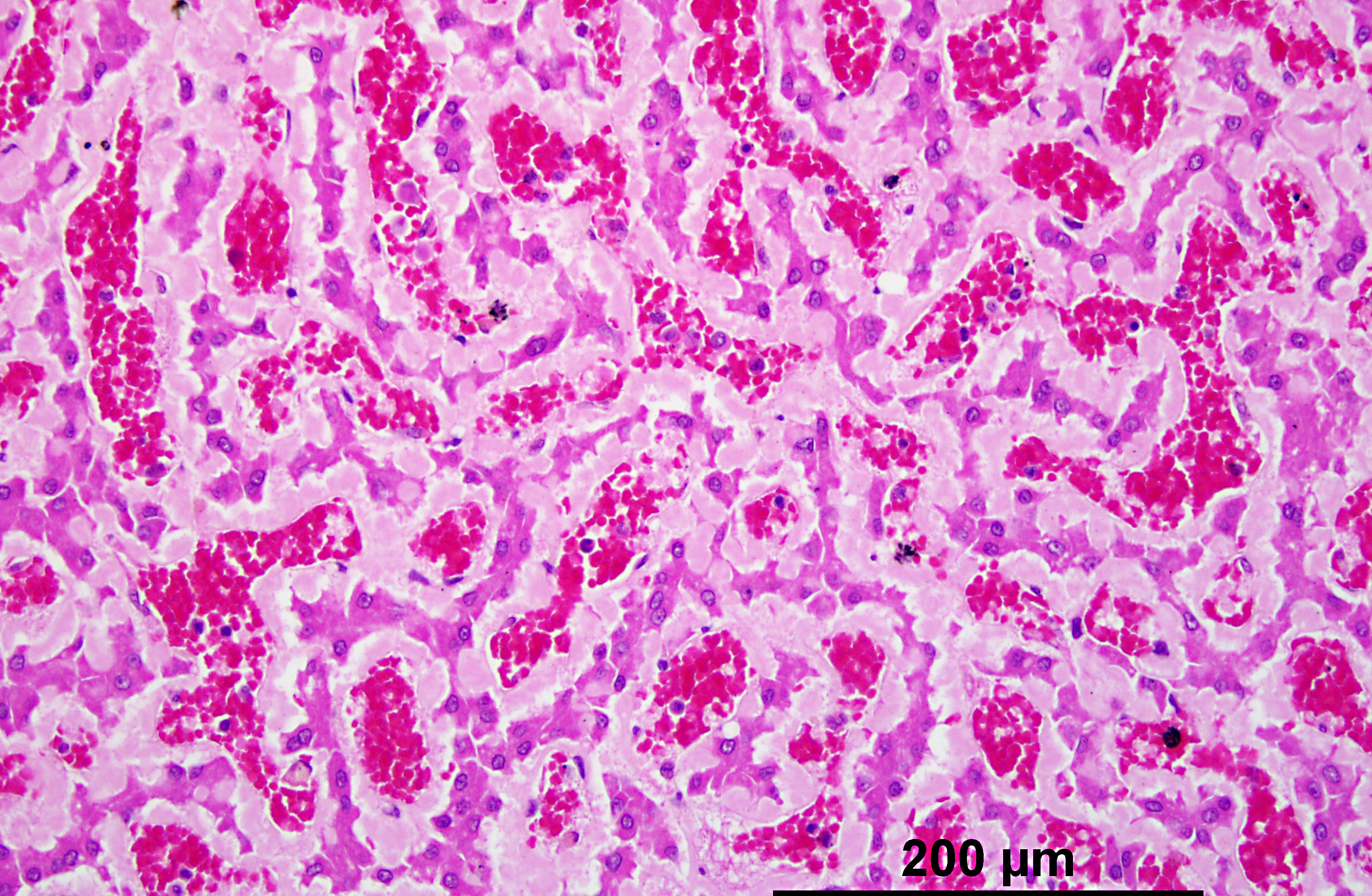
Liver: An abundant amount of amorphous, eosinophilic, homogeneous, extracellular material interpreted as amyloid is deposited diffusely in the space of Disse and encroaches on adjacent hepatic parenchymal cells and sinusoids. There is multifocal deformity, pressure atrophy and disappearance of hepatocytes, causing total replacement of large areas of liver parenchyma. There is a small amount of the same material in the vessel walls of few portal areas.
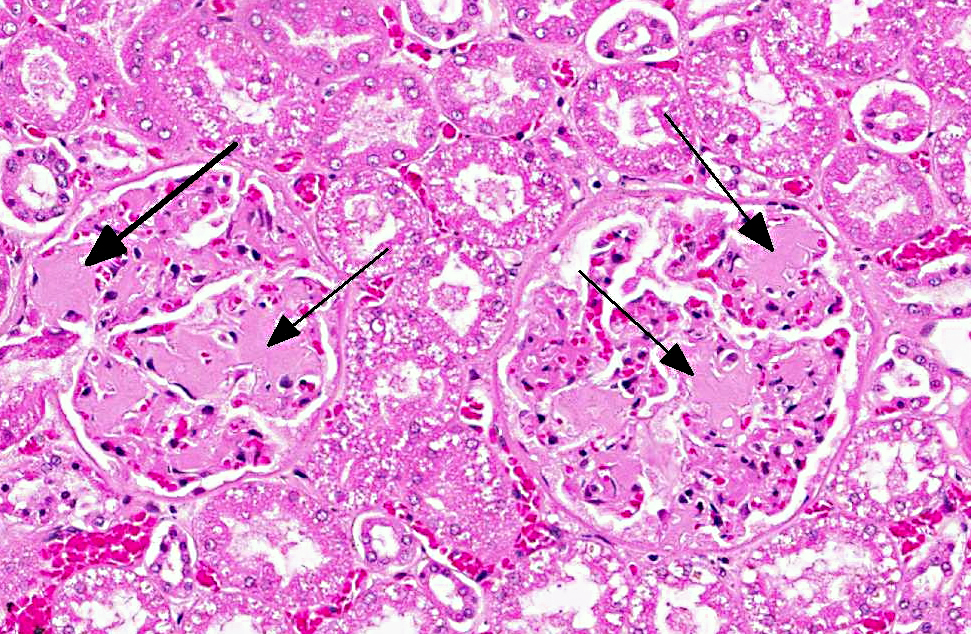
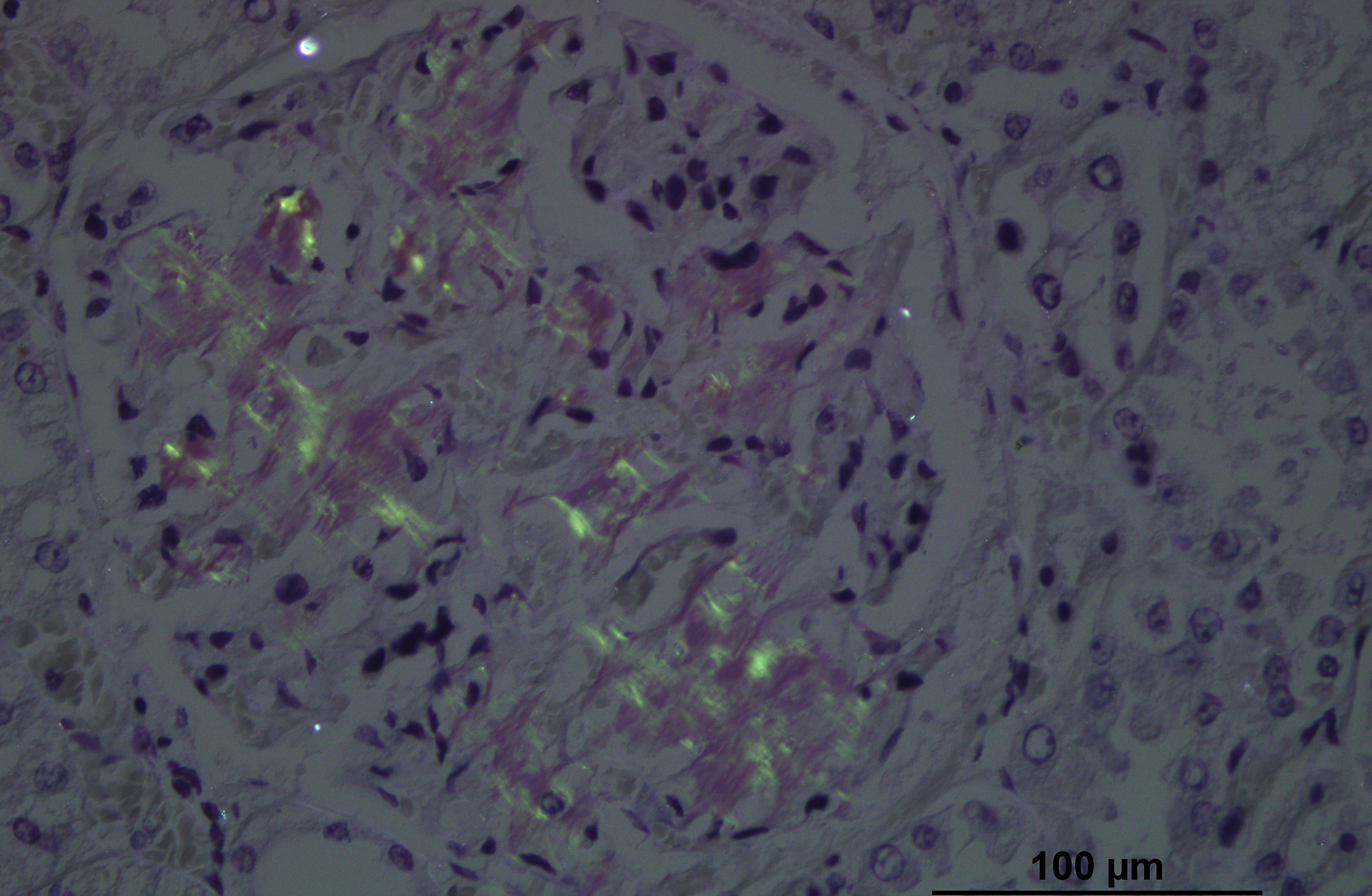
Kidney: In all glomeruli, there is a segmental to diffuse, moderate to abundant amount of amorphous, eosinophilic, homogeneous, extracellular material in the mesangial area and in the subendothelium of glomerular capillaries. The depositions gradually develop until the glomeruli, when entirely involved, are enlarged and appear as hypocellular, eosinophilic, homogeneous spheres in which the capillaries are obliterated. With Congo red, amyloid is stained a light orange-red. In the medulla, not visible on the slide, the tubules are dilated and contain a striking amount of homogeneous, pink, hyaline casts interpreted as protein (proteinuria).
Morphologic Diagnosis:
1. Liver: Amyloidosis, diffuse, severe.
2. Kidney, glomeruli: Amyloidosis, severe.
Condition:
Contributor Comment:
In the kidney, both glomerular and interstitial medullary deposition have been reported.(1) Additionally, the dog in this case had a small amount of amyloid deposition in the spleen.
Amyloidosis is a group of disorders in which amyloid is deposited in the walls of small blood vessels and extracellularly in a variety of sites, particularly in renal glomeruli. All amyloid fibrils have a β-pleated sheet structure.(5) By light microscopy and standard hematoxylin and eosin staining, amyloid appears as an amorphous, eosinophilic, hyaline, extracellular substance.(6) The histologic diagnosis is usually confirmed with special stains. Amyloid is stained a light orange-red with Congo red, and then exhibits green birefringence in polarized light.(5)
Amyloidosis is seen in a number of presentations:
1. Immunoglobulin-derived (primary, or AL) amyloidosis is the most common form in humans, but it is uncommon in domestic animals. AL amyloid is produced from immunoglobulin light chains in plasma cell dyscrasias as a product of monoclonal B-cell proliferation.(5)
2. Reactive systemic (secondary or AA) amyloidosis is the most common form in domestic animals. AA amyloid is derived from serum protein AA, an acute-phase reactant apoprotein product of hepatocytes predominantly. Serum protein AA is produced in excess as a result of chronic antigenic stimulation, such as occurs in persistent infectious, inflammatory or neoplastic (nonimmunocyte dyscrasias) conditions.(5,7)
3. Familial amyloidosis is a systemic form of AA amyloidosis that is hereditary in some breeds of dogs and cats.(7) AA amyloidosis occurs in Beagles, Shar-Pei dogs, gray Collies, English Foxhounds, Abyssinian cats and Siamese and Oriental cats.
4. Apolipoprotein AI-derived amyloidosis affects the pulmonary vessels of old dogs.
5. Islet amyloid polypeptide-derived amyloidosis is common in the pancreatic islets of cats with non-insulin-dependent diabetes mellitus.(5)
Both AA and AL amyloidosis can occur in either systemic or localized forms. The cause of amyloid fibril formation and deposition is obscure, but the nidus theory postulates that amyloid fibrils serve as templates for fibril growth and as scaffolding for fibril polymerization. Amyloid-enhancing factor may be involved.(5)
JPC Diagnosis:
1. Liver, space of Disse: Amyloidosis, diffuse, severe, with cholestasis and hepatocyte atrophy and loss.
2. Kidney, glomeruli: Amyloidosis, segmental to global, diffuse, marked, with scattered tubular degeneration and necrosis.
Conference Comment:
The location of amyloid deposits varies based on the pathogenesis and the species affected. Overall, the kidney is the most common site for amyloid deposition in many domestic species, with the glomeruli being most frequently affected in most domestic species, except the cat where medullary interstitial deposition of amyloid is more common. The space of Disse in the liver is also a common site for amyloid deposition in birds, cattle, horses, dogs and cats. The spleen is a frequent site in reactive systemic amyloidosis, with amyloid deposits occurring in the periarteriolar lymphoid sheaths and red pulp. Organs affected in localized amyloidosis include the skin and nasal septum and turbinates in horses and pancreatic islets of Langerhans in cats.(6)
Clinocopathologic consequences of renal amyloidosis include the nephrotic syndrome, which is characterized by the tetrad of hypercholesterolemia, proteinuria, hypoproteinemia, and generalized edema. Additionally, a urine-protein-to-urine-creatinine ratio (UP/UC) greater than 18 is associated with renal amyloidosis. Ultrastructually, amyloid fibrils are non-branching, 7.5 to 10 nm in diameter, and lack the periodicity which is characteristic of fibrin and collagen diameter tubules by electron microscopy.(7)
There was some slide variation, with some slides having only the section of kidney.
References:
2. DiBartola SP, Tarr MJ, Webb DM, Giger U. Familial renal amyloidosis in Chinese Shar Pei dogs. J Am Vet Med Assoc. 1990;197(4):483-7.
3. Loeven KO. Hepatic amyloidosis in two Chinese Shar Pei dogs. J Am Vet Med Assoc. 1994;8:1212-16.
4. Loeven KO. Spontaneous hepatic rupture secondary to amyloidosis in a Chinese Shar Pei. J Am Anim Hosp Assoc. 1994;30:577-79.
5. Maxie MG, Newman SJ. Glomerular disease: Amyloidosis. In: Maxie MG, ed. Jubb, Kennedy, and Palmers Pathology of Domestic Animals. 5th ed. Philadelphia, PA: Saunders Elsevier; 2007:463-65.
6. Myers RK, McGavin MD, Zachary JF. Cellular adaptations, injury and death: morphologic biochemical and genetic bases. In: McGavin MD, Zachary JF, eds. Pathologic Basis of Veterinary Disease. 5th ed. St Louis, MO: Elsevier Mosby; 2012:36-38.
7. Snyder PW. Diseases of immunity: Amyloidosis. In: McGavin MD, Zachary JF, eds. Pathologic Basis of Veterinary Disease. 4th ed. St. Louis, MO; Mosby Elsevier; 2007:246-51.
8. Tripathi NK, Gregory CR, Latimer KS. Urinalysis. In: Latimer KS, ed. Duncan & Prasses Veterinary Laboratory Medicine Clinical Pathology. 5th ed. Ames, Iowa: Wiley-Blackwell; 2011:253-282.