Signalment:
More recent clinical presentation was for an ulcerated lip mass which had been noted for eight weeks. The owners also described that the cat had been wandering around the house, stuck in small spaces, was incoordinated, stumbling and vocalizing, with a decreased appetite. On physical exam, there were multifocal neurologic signs including decreased menace bilaterally, positional nystagmus and inappropriate mentation. Additional findings included left retinal detachment, heart murmur and thickened intestines with palpation.
Gross Description:
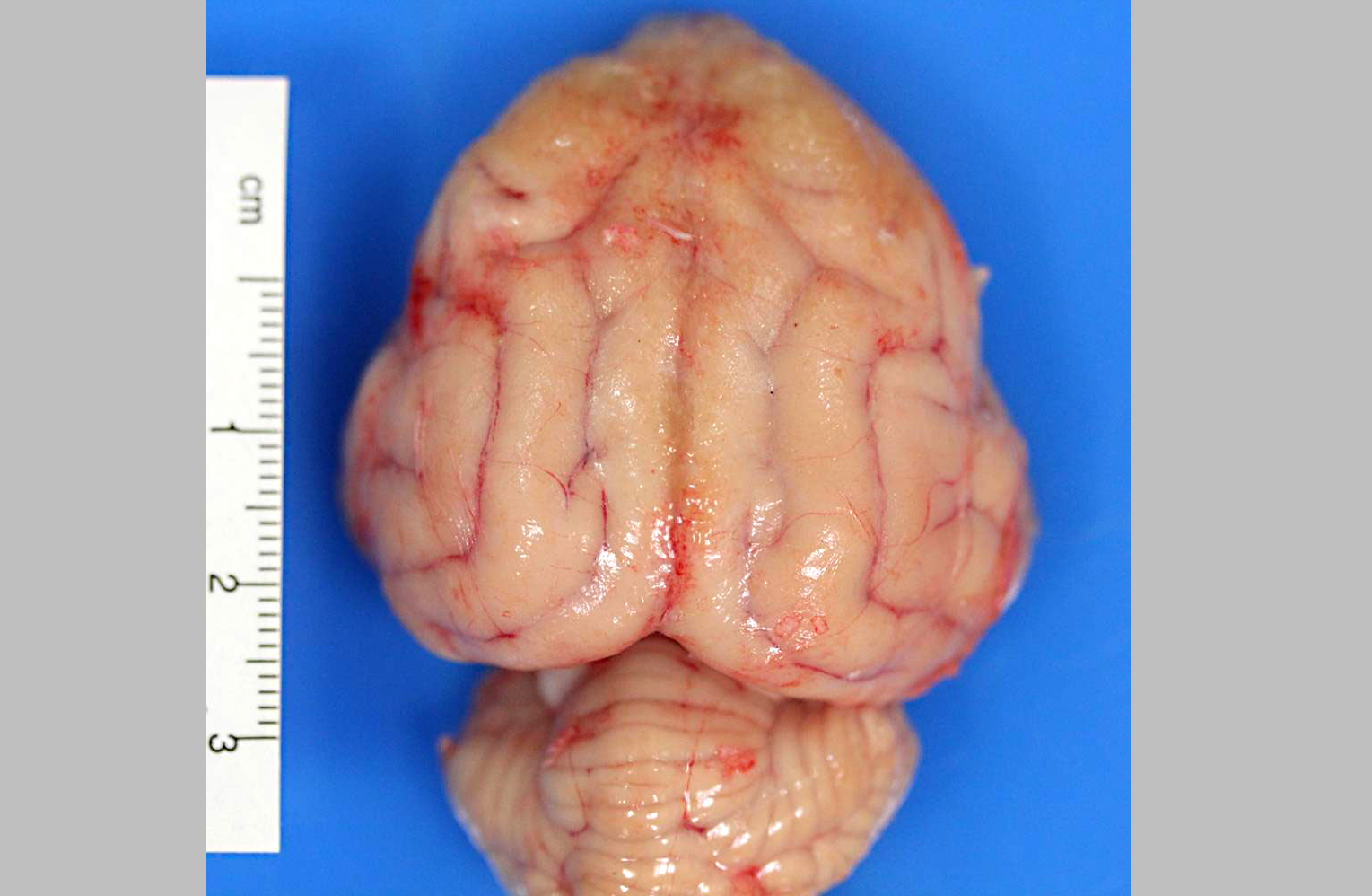
The vermis of the cerebellum is focally compressed and flattened against the underlying brainstem at the foramen magnum (herniation). The leptomeninges of the rostral and dorsal cerebrum are thickened by granular, irregular, yellow to tan material (meningitis). When the fixed brain is sectioned, there is marked leptomeningeal expansion by similar granular material, with adherence of the right and left hemispheres of the rostral cerebrum at the longitudinal cerebral fissure.Â
Histopathologic Description:
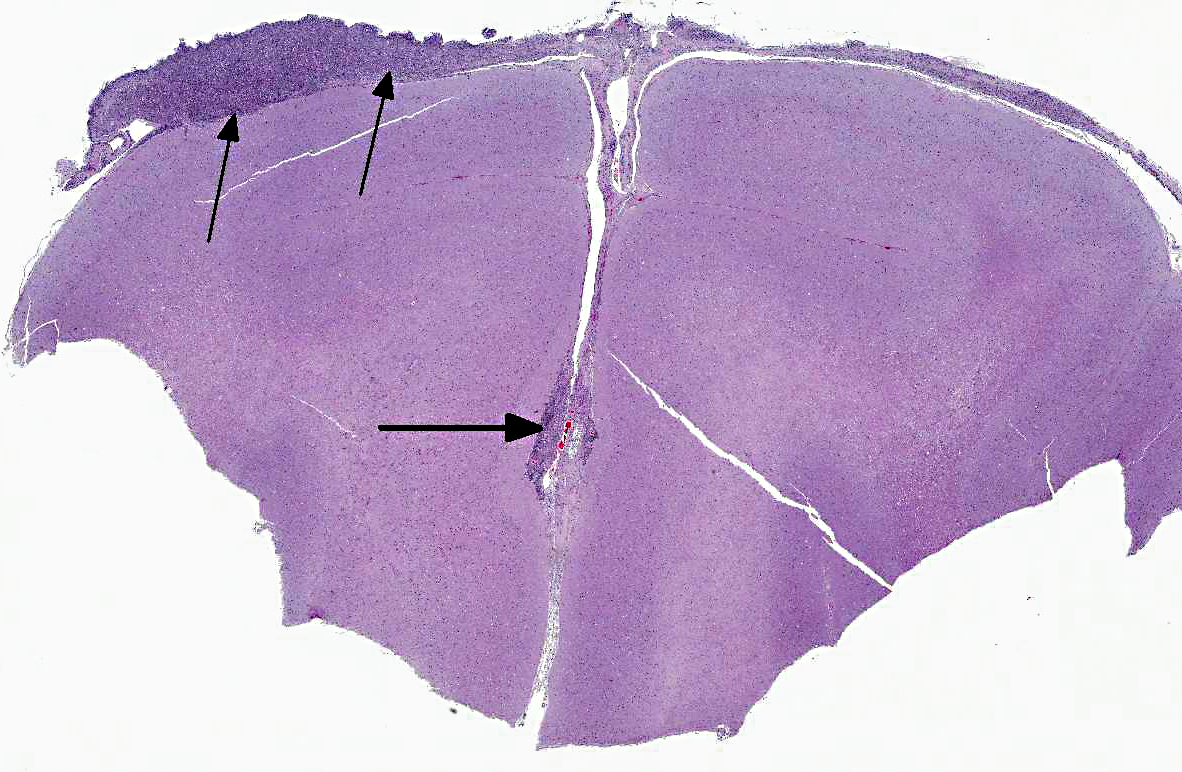
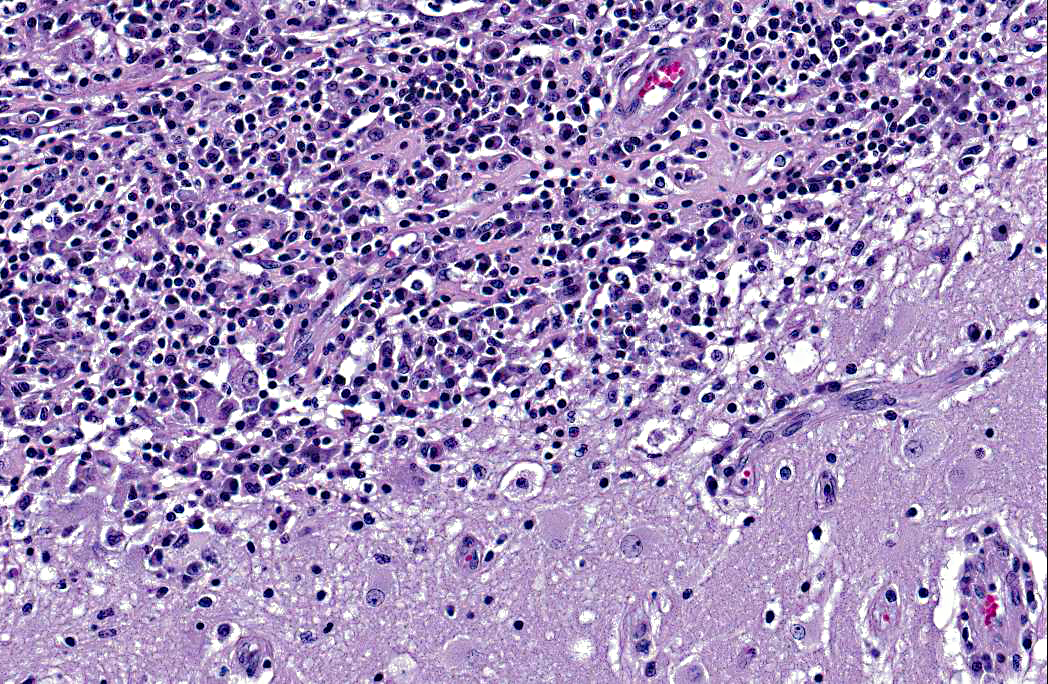
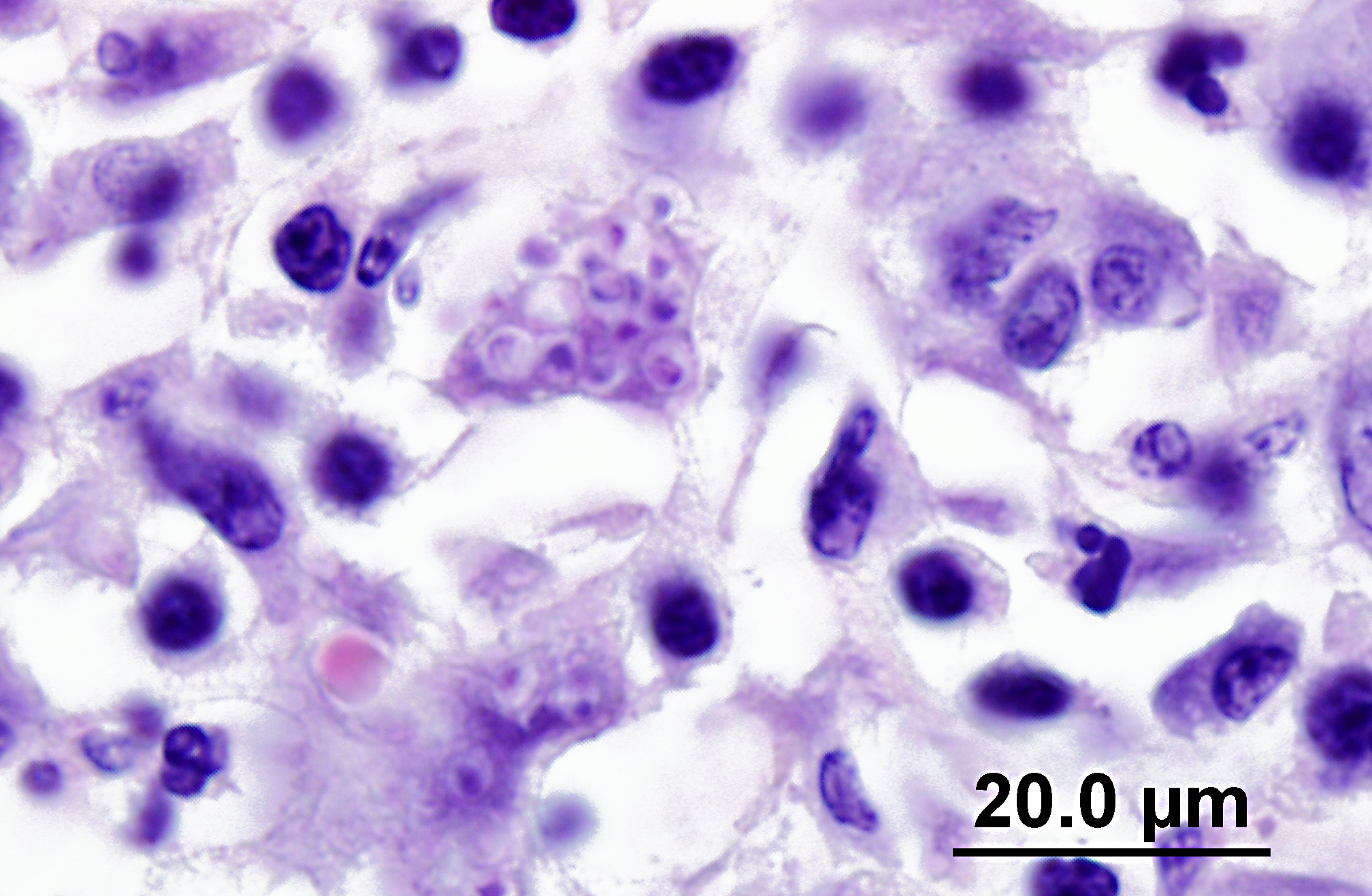
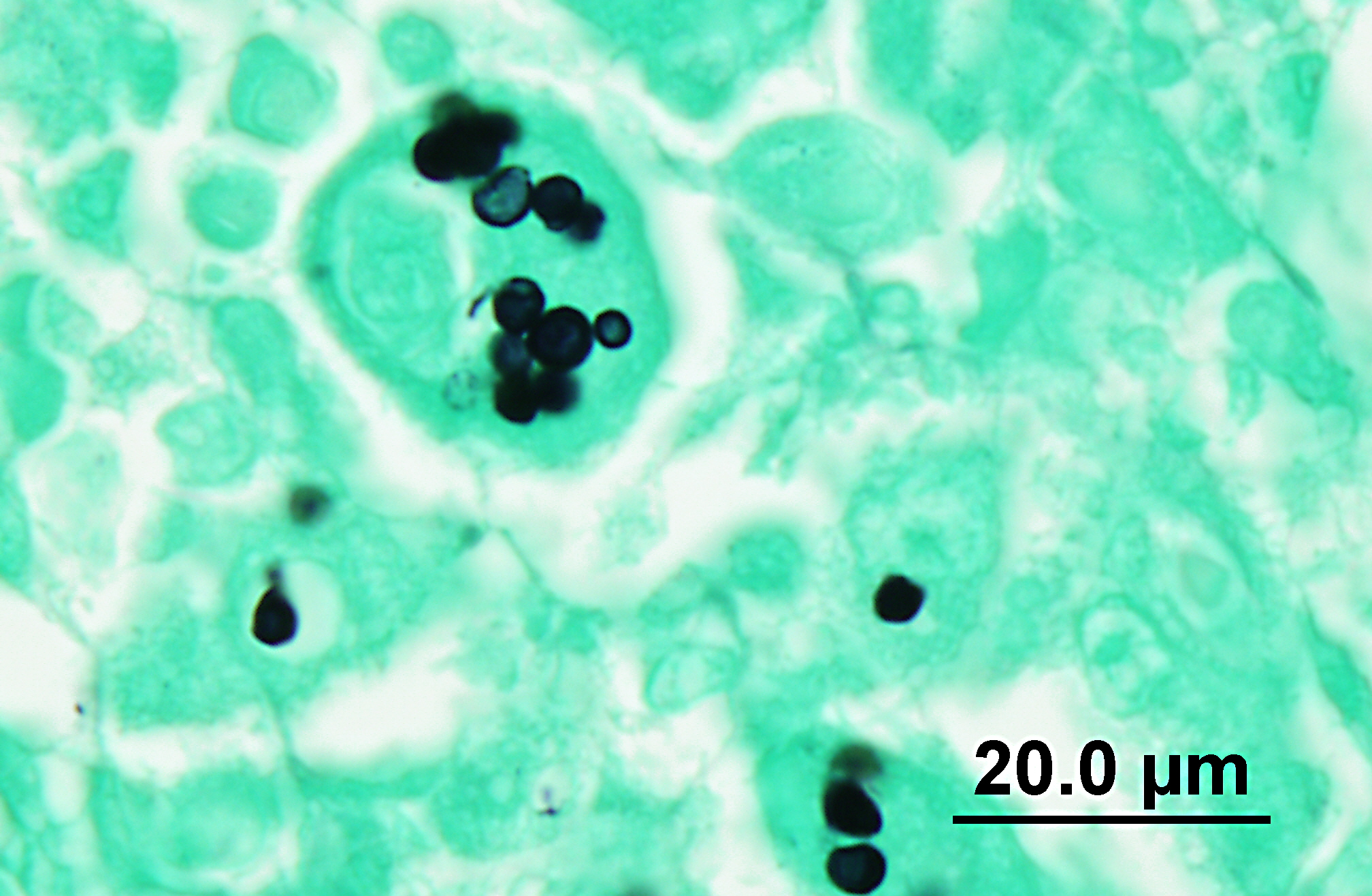
Histoplasma immunohistochemistry (provided by the University of Connecticut Veterinary Medical Diagnostic Laboratory): Brain: Multifocally throughout the meninges, within macrophages, there are numerous positive staining, intracellular, spherical, 3-4 μm diameter organisms (Histoplasma capsulatum).
Similar, positive staining organisms are identified in the previous bone biopsy, lungs, adrenal glands and eye.
Morphologic Diagnosis:
Lab Results:
Cytology: Aspirate of mass from the right lower lip region: All slides are examined and are found to be similar; the specimen is of moderate cellularity and contains moderate numbers of red blood cells with low to moderate numbers of nondegenerate neutrophils and activated macrophages. Rare tissue cells are identified and these are uniform fibrocytes showing no evidence of dysplasia or atypia. On several of the slides there are extremely low numbers of intracellular yeast structures; these are 1-3 microns in diameter, round to oval with a variably thick capsule and are primarily found within the cytoplasm of very few of the macrophages. The yeast organisms most resemble Histoplasma sp.Â
Microscopic interpretation: Mild to moderate mixed (neutrophilic and histiocytic) inflammatory infiltrate associated with intracellular yeast organisms.Â
Comment: Although the numbers of yeast structures are quite low, they provide unequivocal evidence of a primary fungal etiology and are most characteristic of Histoplasma capsulatum.
Condition:
Contributor Comment:
A retrospective study of 22 cases of feline histoplasmosis found that amongst three categories (disseminated, pulmonary and gastrointestinal), disseminated was the most common manifestation, occurring in 68% of cases. The most frequent sites of infection were listed as the lungs, lymph nodes, liver, spleen, kidney, adrenal glands, eyes, bone marrow and the gastrointestinal tract.(1) Disseminated infection with involvement of the brain is rarely reported in cats and dogs.(4,7,9) In this case, the brain was the most severely affected organ, and the cat re-presented for its neurologic signs. Immunohistochemistry for Histoplasma was performed at the University of Connecticut Veterinary Medical Diagnostic Laboratory. The combination of H&E, silver stains and IHC confirmed Histoplasma organisms in the brain, eye, lungs, adrenal glands, bone marrow at site of previous surgery (taken at the time of surgery) and the ulcerated lip lesion. Demonstrable organisms in the ulcerated lip lesion correlated with the cytologic results. In one report, a review of cases from the authors institution revealed that several cats with oral histoplasmosis presented with focal or multifocal exophytic or ulcerative lesions within the oral cavity, with no apparent systemic involvement.(6) Osseous lesions with associated soft tissue swelling or joint effusion and lameness have been described with feline histoplasmosis.(3) Histoplasma organisms were immunohistochemically identified in the bone marrow biopsy obtained 5 months before euthanasia, indicating a long time frame of infection. Although the intestines were palpably thickened, neither granulomatous enteritis nor intralesional organisms were identified at postmortem examination; however, the intestines displayed mucosal fibrosis, which may indicate previous infection.Â
The cat in this case had a history of being indoor-only for 3 years, and prior to this had intermittent access to the outdoors in rural Pennsylvania. Other reports of histoplasmosis in indoor only cats without travel to endemic regions suggest that household dust or potting soil are possible sources of infection.(3) Some studies found a high prevalence of FeLV in cats with the disseminated form of histoplasmosis, whereas others found a low prevalence.(1,4) In our case, the cat was negative for both FIV and FeLV. Typical clinicopathologic changes in cats with disseminated histoplasmosis include normochromic, normocytic, nonregenerative anemia, hypoalbuminemia, and thrombocytopenia, with variable leukocyte counts.(3,4) Nonregenerative anemia is suspected to result from chronic inflammatory disease, Histoplasma infection of the bone marrow, and intestinal blood loss in gastrointestinal disease. Some cats have been reported to have hyperproteinemia, hyperglobulinemia, mild hyperglycemia or hyperbilirubinemia, and elevations of alanine aminotransferase activities. Hypercalcemia has been reported in several cats and is likely due to granulomatous disease.(3) In our case, mild elevations of ALT and AST may be explained by concurrent chronic cholangiohepatitis.
JPC Diagnosis:
Conference Comment:
References:
2. Br+�-�mel C, Greene CE: Histoplasmosis. In: Greene CE, ed. Infectious Diseases of the Dog and Cat. 4th ed. St Louis, MO: Elsevier Saunders; 2012:614-621.
3. Br+�-�mel C, Sykes JE. Histoplasmosis in dogs and cats. Clin Tech Small Anim Pract. 2005;20(4):227-32. Review.
4. Clinkenbeard KD, Cowell RL, Tyler RD. Disseminated histoplasmosis in cats: 12 cases (1981-1986). J Am Vet Med Assoc. 1987;190(11):1445-1448.
5. Gades NM, Marler RJ. Pathology in practice. J Am Vet Med Assoc. 2009;234(12):1535-1537.
6. Lamm CG, Rizzi TE, Campbell GA, Brunker JD. Pathology in practice. Histoplasma capsulatum infections. J Am Vet Med Assoc. 2009;235(2):155-7.
7. Lavely J, Lipsitz D. Fungal infections in the central nervous system in the dog and cat. Clin Tech Sm Anim Prac. 2005;20:212-219.
8. Quinn PJ, Markey BK, Leonard FC, FitzPatrick ES, Fanning S, Hartigan PJ. Dimorphic fungi. In: Veterinary Microbiology and Microbial Disease. 2nd ed. Ames, Iowa: Blackwell Science Ltd; 2011: Kindle edition.Â
9. Schaer M, Johnson KE, Nicholson AC. Central nervous system disease due to histoplasmosis in a dog: a case report. J Am Anim Hosp Assoc. 1983;19:311-315.