Signalment:
4-year-old, male, Labrador retriever dog (
Canis familiaris) An outbreak of severe illness and death affected 181 dogs in an animal shelter starting in August, 2008
and subsided in January, 2009. Clinically, the dogs progressively developed signs of vomiting, anorexia, depression,
icterus, ascites, melena, hematochezia or hematemesis, and eventually death. All dogs received vaccination and
deworming for endo/ectoparasites. They were fed a commercialized dog food. PCR results for
Leptospira sp.,
parvovirus, adenovirus,
Ehrlichia sp., and
Babesia sp. were all negative. Analysis for organic phosphorus and
cyanide in intestinal contents was also negative. Based on the presentation and preliminary laboratory results,
intoxication was suspected by the clinicians.
Gross Description:
The dog was severely icteric with marked yellow discoloration on mucous membranes, skin,
sclera, and adipose tissue. The abdominal cavity contained approximately 970 ml of a yellow to dark orange,
translucent, watery fluid (ascites). There were a few fibrin strings adherent to the intestinal serosa.. The liver was
slightly enlarged, diffusely yellow-tinged and firm with locally extensive white irregular, scar-like areas. The gall
bladder wall was thickened with marked submucosal edema. There were multifocal to coalescing, red foci
(hemorrhage) scattered on the gastrointestinal tract, urinary bladder, pancreas, and heart. The intestines contain
small to moderate amounts of dark red, tarry contents. Aside from the hemorrhage, the urinary bladder was diffusely
yellow. Lungs were diffusely reddened, wet and heavy. Bronchi were filled with frothy fluid. Both kidneys were
slightly enlarged, and the medulla was yellowish on cut surfaces.Â
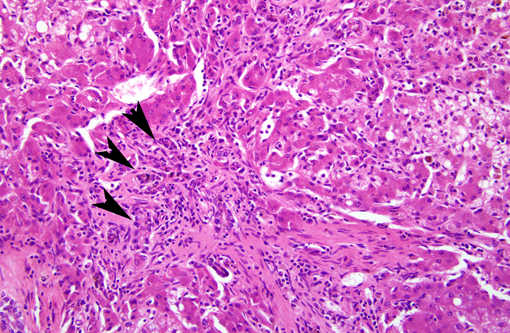
Histopathologic Description:
Liver: The surface of the liver is irregular and the lobules become indistinct and
irregular. The lobules are characterized by variable hepatocellular hydropic degeneration, lipidosis, and necrosis,
biliary hyperplasia, and portal, periportal to bridging fibrosis. The remaining hepatocytes display cellular atypia and
regeneration characterized by variably sized and shaped cells and nuclei. Scattered binucleated and multinucleated
hepatocytes are also noted. Along with these changes, there is also diffuse moderate to severe inflammation
characterized by locally extensive infiltration of macrophages, neutrophils, fewer plasma cells and lymphocytes
accompanied with variable fibrosis. Mild to moderate bile stasis is diffusely present. Yellow to brown pigment-
ladened macrophages and Kupffer cells are also frequently seen.Â
Morphologic Diagnosis:
Liver: Hepatocellular fatty change and regeneration, severe, with hepatitis,
chronic-active, moderate; portal, periportal, and bridging fibrosis; bile duct hyperplasia; and cholestasis.Â
Lab Results:
Aflatoxins were detected from the commercial canine food consumed by the affected dog. The
concentration of aflatoxin B1 in this commercial canine food was over 150 ppb examined by Animal Health
Research Institute and T+�-�V Rheinland Aimex Ltd. PCR results for
Leptospira sp., parvovirus, adenovirus,
Ehrlichia
sp., and
Babesia sp. were all negative. Analysis of intestinal contents for organic phosphorus and cyanide were also
negative.Â
Condition:
Aflatoxicosis
Contributor Comment:
Aflatoxins are a group of related, natural, toxic byproducts of the fungi
Aspergillus
flavus, Aspergillus parasiticus, and a new select
Penicillium spp. Aflatoxin B1 is the most hepatotoxic, and also can
be immunosuppressive, nephrotoxic, and carcinogenic, as well as cause hemolytic anemia and coagulopathies.Â
Aflatoxins are liposoluble and readily absorbed from the gastrointestinal tract into the portal blood. They are then
transported to the liver for metabolism. Toxicosis is a result of binding of essential enzymes, which blocks DNA
polymerase and ribosomal translocase and leads to the formation of DNA adducts.Â
It has been suggested that the carcinogenic action of aflatoxin B1 in the rat results from a capacity to bind to DNA, a
characteristic similar to that of actinomycin D. However, lethal doses of actinomycin D do not produce hepatic
parenchymal cell necrosis. In all species studied, the organ most affected is the liver, although other organs,
particularly the kidney, show signs of damage. The distribution of the hepatic lesion is not consistent from species to
species, i.e., rat and duckling, periportal; guinea pig and swine, centrilobular; dog, periportal and centrilobular; and
rabbit, mid-zonal. In contrast, most other hepatotoxins, such as carbon tetrachloride, regularly induce a centrilobular
lesion in both rats and guinea pigs. There is a wide range in the acute LD dose of aflatoxin B1, varying from 0.3
mg/kg for ducklings to 16 mg/kg for mature female rats. In species for which data are available, the young appear to
be more susceptible than mature animals. Although the Food and Drug Administration suggests a zero tolerance for
aflatoxin in food, it lists a legal limit of 20 mg/kg (ppb) in feed. For dogs, the lethal dose, 50% (LD50) value is just
500 to 1,000 mg/kg (ppb), and, 60 mg/kg (ppb) is a toxic dose.Â
In the present cases from the Bali shelter, at necropsy these dogs fed commercial dog feed containing aflatoxic
peanut meal were jaundiced with swelling and yellowish discoloration of the liver and edema of the gall bladder
identical to that seen with crude or purified aflatoxin. The causes of death are believed mainly to be due to severe
hepatic damage and the subsequent secondary coagulation defect. The insufficient production of coagulation factors
due to severe hepatic injury induces hemorrhages in multiple organs and tissues, including heart, gastrointestinal
tract, kidney, pancreas, and adipose tissue. The order of severity and histopathology are variable between different
cases, because the varying rates of metabolism between different species, ages, nutritional status and hormone levels
hinder assessment of exposure in animals. Additionally, the susceptibility of individual dogs can be affected by
levels of sex hormones, age, dose, and/or degree of feed refusal.Â
JPC Diagnosis:
Liver: Macronodular hepatocellular regeneration, diffuse, severe with microvesicular steatosis,
necrosis, cholestasis, bridging portal fibrosis, and biliary hyperplasia (ductular reaction type 1.).Â
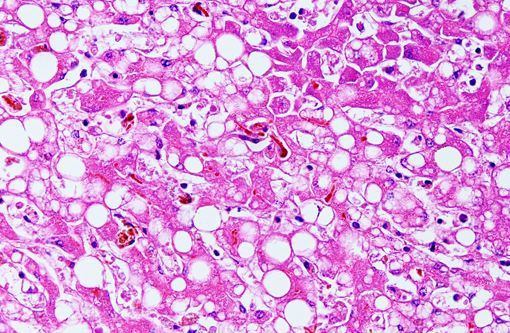
Conference Comment:
Histologic features of prominent fatty degeneration, bridging fibrosis, and severe
cholestasis, marked by bile pigment within hepatocyte cytoplasm (fig) are common features of a number of
hepatotoxicities, including phenobarbitol intoxication, copper toxicosis, low-grade chronic microcystin toxicity,
certain homeopathic herbal mixtures and chronic aflatoxicosis as in this case,. Acute aflatoxicosis, by contrast, is
characterized by hemorrhage, severe fatty change, and biliary hyperplasia.Â
Another important histologic feature is that many portal areas have diminutive portal veins or lack them altogether.Â
This is presumably secondary to portal hypertension from the massive dissecting fibrosis, which prohibits adequate
downstream perfusion of portal veins and venules.Â
References:
1. Bingham AK, Huebner HJ, Phillips TD, Bauer JE. Identification and reduction of urinary aï¬atoxin metabolites in
dogs.Â
Food Chem Toxicol. 42: 1851-1858, 2004.Â
2. Newman SJ, Smith JR, Stenske KA, Newman LB, Dunlap JR, Imerman PM, Kirk CA. Aflatoxicosis in nine dogs
after exposure to contaminated commercial dog food.
J Vet Diagn Invest. 19:168-175, 2007.Â
3. Stanworth SJ, Hyde CJ, Murphy MF. Evidence for indications of fresh frozen plasma.Â
Transfus Clin Biol. 14:
551-556, 2007.Â