Signalment:
13 year castrated male Quarter horse, Equus caballusMultiple subcutaneous masses in the lateral aspect of both right and left proximal forearms. These lesions appeared within the past 6 months. Lesions are not apparently painful and there is no associated lameness or other clinical signs. The horse is heterozygous for the hyperkalemic periodic paralysis mutation. A portion of each lesion was excised and submitted for histopathology. No association with underlying skeletal muscle was detected at surgery.
Gross Description:
Discrete firm pale tan nodular masses with normal overlying haired skin.
Histopathologic Description:
Two wedge samples, one from the right foreleg and one from the left foreleg, were submitted and representative sections were submitted for histopathology. Both lesions are similar and are composed of haired skin with underlying cutaneous skeletal muscle (presumed cutaneous omobrachialis, although the site appears slightly more distal than anatomy texts describe for insertion of this muscle in the horse). Architecture of the skeletal muscle is markedly distorted to effaced, with expansion to form irregular nodular masses. Myofibers within the masses exhibit varying degrees of the following changes:
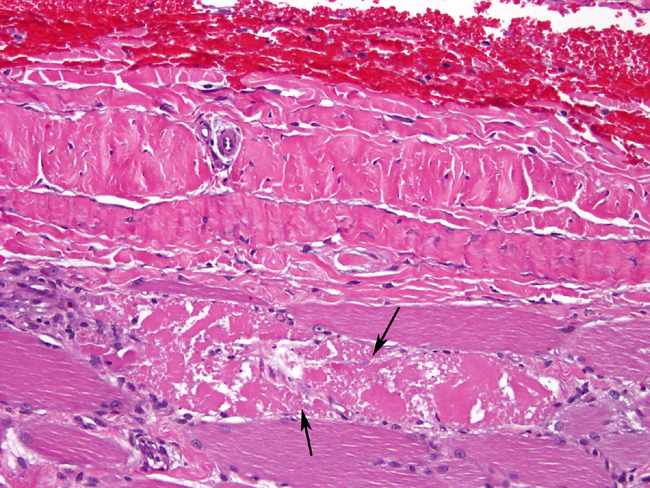
- Disarray of orientation, with some fibers in transverse section, others in longitudinal section, and still others in oblique section.
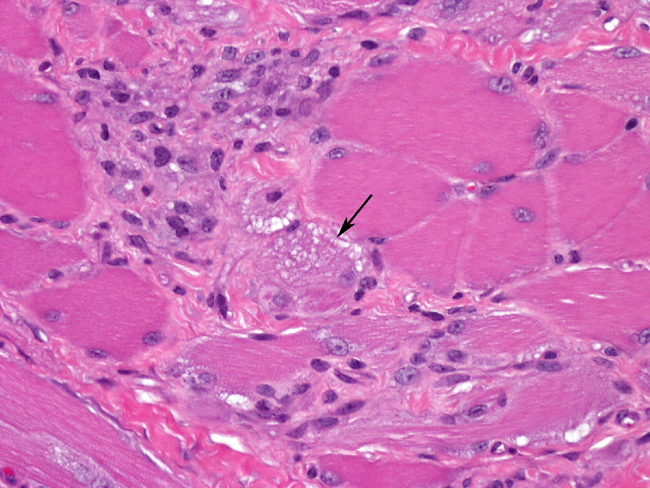
- Severe chronic myopathic change, including marked variation in fiber size with fiber hypertrophy and also rounded to angular atrophy, endomysial and perimysial fibrosis, internal nuclei, fiber splitting, and subsarcolemmal pale zones containing pale pink to gray finely granular material (sarcoplasmic masses).
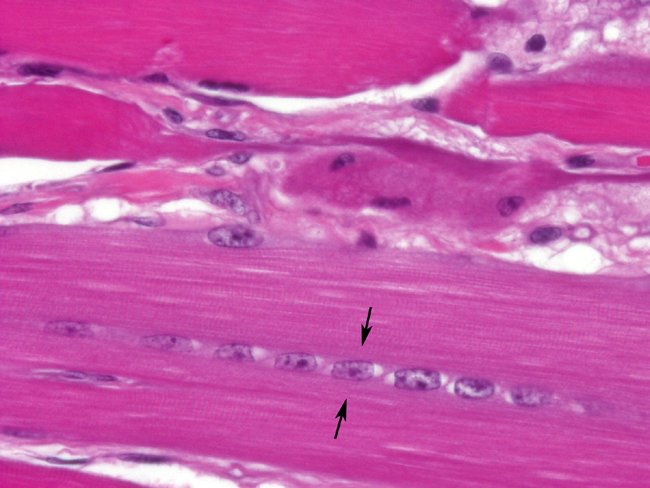
- Degenerative and regenerative changes, including segmental coagulation necrosis often with macrophage infiltration and vacuolar degeneration. Small diameter, slightly basophilic fiber segments with prominent euchromatic nuclei often in clusters or short chains - are indicative of myofiber regeneration.
- Multifocal, typically mild to moderate, interstitial infiltrates of lymphocytes.Â
Massons trichrome stain confirms the presence of endomysial and perimysial fibrosis. Sarcoplasmic masses and vacuoles do not stain with either trichrome stain or Periodic acid-Schiff stain for glycogen, and no abnormal glycogen aggregates are present.
Morphologic Diagnosis:
Skeletal muscle, cutaneous omobrachialis: Pseudotumor consistent with focal myositis
Condition:
Muscular pseudotumor
Contributor Comment:
The term muscle pseudotumor encompasses a group of benign non-neoplastic processes causing mass lesions within skeletal muscle.1-5 The muscle pseudotumors recognized to date in animals are myositis ossificans, musculoaponeurotic fibromatosis (desmoid tumor), and fibrotic myopathy in horses, and myositis ossificans and a lesion simply termed muscle pseudotumor in dogs. The latter lesion is characterized by profound myopathic changes, interstitial connective tissue infiltration, mild to moderate myofiber necrosis and regeneration, and a variable degree of inflammation, most often lymphocytic. 2 These features are also typical of the muscle pseudotumor reported as focal myositis in people.1,3-5 Diagnosis of any muscle pseudotumor relies on a clinical history of a nodular mass within skeletal muscle, with no other neuromuscular or systemic disease signs, as in the absence of this history a diagnosis of muscular dystrophy, chronic denervation atrophy, or chronic myositis is possible.
Muscle pseudotumors in people occur most often in limb muscle, although other sites are possible. Patients describe these lesions as either non-painful or as being associated with mild discomfort or dull pain.1,3-5 Although trauma has been proposed as a cause, careful case studies of affected people have not detected a history of prior trauma to the area.1,3-5 Subclinical muscle tearing has been speculated to be a possible cause.3 Evidence of peripheral nerve damage has been detected within some muscle pseudotumors in people, but is not common and is thought to be a secondary event rather than a primary cause.4 There is no apparent age or gender predisposition in people.1,3-5
In people, muscle pseudotumors must be differentiated from localized initial forms of polymyositis.5 No such association has been identified in animals. This horse was otherwise clinically normal, and the history of being heterozygous for hyperkalemic periodic paralysis was not considered to be related to the development of these lesions. It is curious that this case occurred bilaterally, in what appears to be the distal cutaneous omobrachialis muscle, in a lateral location that is less likely to be traumatized than cranial areas. Similar to case studies of focal myositis in people, there was no history of trauma to this area.
Muscle pseudotumors in animals have not been described as being associated with pain. Locations include within limb muscle,2 as in this case, but these lesions have also been seen in scapular2 and laryngeal muscle (unpublished observations). In pseudotumors of dogs and horses that this contributor has studied, lymphocytic inflammation is extremely variable and often not prominent. A similar situation is described in people with focal myositis.1,3 An additional characteristic histopathologic finding in focal myositis-like muscle pseudotumors in animals, apparently not described in human cases, is prominent disarray of myofiber arrangement, with the finding of transverse, longitudinal, and obliquely arranged myofibers within the same section.2
Surgical excision of these lesions is curative in people and also in animals. Progression beyond the initial growth phase, which can be rapid, is not described.1,3-5 In this current case only portions of the lesions had been excised at the time of this submission. Follow up is planned in order to determine future behavior.
JPC Diagnosis:
Haired skin and skeletal muscle, cutaneous omobrachialis (per
contributor): Myocyte proliferation, focally extensive, moderate, with myofiber disarray,
degeneration, necrosis, atrophy, hypertrophy and regeneration, interstitial fibrosis, and
mild lymphohistiocytic inflammation (focal myositis), Quarter Horse, equine.
Conference Comment:
The contributor provides a thorough review of muscle
pseudotumors in dogs and horses. Not much is known about this idiopathic condition,
and without knowledge of clinical history, or gross images, it is a difficult diagnosis to
make. It is thought that focal myositis, myositis ossificans, and musculoaponeurotic
fibromatosis (desmoid tumor) arise from an abnormal response to muscle trauma, while
fibrotic myopathy results from a denervation injury. There was a small amount of
variability in the amount of fibrosis and inflammation among slides. Several slides
contained areas with a high mitotic rate, which were interpreted as areas of intense
regeneration. No infectious organisms were seen on special stains performed at AFIP
[Brown & Brenn (B&B), Brown & Hopps (B&H), Gomoris methenamine silver (GMS),
Periodic acid-Schiff (PAS), Ziehl-Neelsen (ZN)].
This case presents great examples of the histologic changes in skeletal muscle
response to injury. Degenerating muscle is swollen with pale vacuolated sarcoplasm.
Necrotic muscle fibers are shrunken and hypereosinophilic, with a loss of crossstriations,
and may be fragmented. Regenerative muscle has basophilic sarcoplasm
with multiple centralized and linearly-arranged nuclei (nuclear rowing). They are often
surrounded by an increased number of satellite cells. Other common changes include
atrophy, hypertrophy and fibrosis. The myofiber disarray is a characteristic lesion of
focal myositis/muscle pseudotumor in horses and dogs, and along with the clinical
history, helps distinguish it from other causes of skeletal muscle degeneration and
necrosis.
References:
1. Colding-J+�-+rgensen E, Laursen H, Lauritzen M: Focal myositis of the thigh: report of two cases. Acta Neurol Scand 88:289-292, 1993
2. Cooper BJ, Valentine BA: Muscle pseudotumors. In: Tumors in Domestic Animals, ed. Meuten DJ, 4th ed, pp. 359-361. Iowa State Press, Ames, IA, 2002
3. Heffner RR, Armbrustmacher VW, Earle KM: Focal myositis. Cancer 40:301-306, 1977
4. Heffner RR, Barron SA: Denervating changes in focal myositis, a benign inflammatory pseudotumor. Arch Pathol Lab Med 104:261-264, 1980
5. Vercelli-Retta J, Ardao G, De Cabrera M: Focal myositis and its differential diagnosis. A case report and review of the literature. Ann Pathol 8:54-56, 1988