WSC 2023-2024, Conference 15, Case 3
Signalment:
4-year-old, female spayed Standard poodle dog (Canis familiaris)
History:
A pilomatrixoma was excised from this animal’s tail base two years prior to presentation for non-weight bearing lameness on the right pelvic limb. Polyostotic aggressive bone lesions were seen on survey radiography. Staging identified pulmonary nodules.
Gross Pathology:
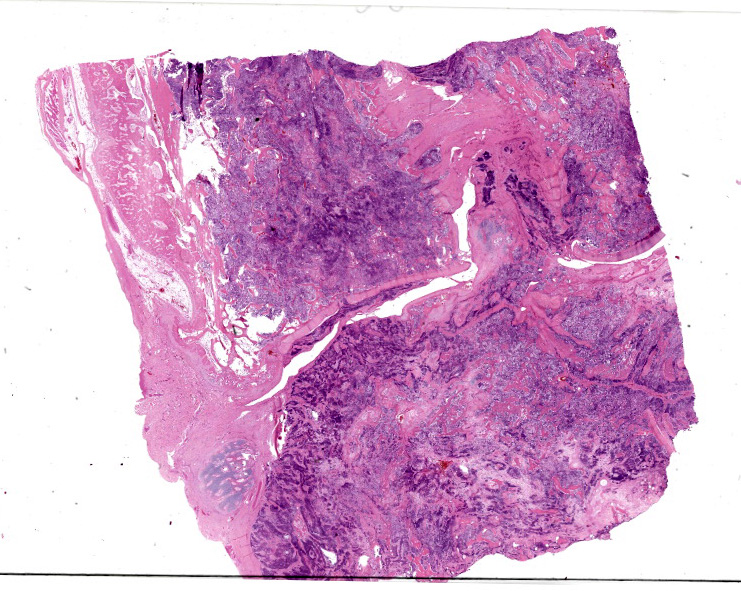
The right hock is circumferentially expanded by a hard, round mass. There is a mass involving the tarsal bones and the metatarsals. There is marked periosteal new bone formation of the distal tibia. There are multiple 1-5 cm nodules throughout the lungs.
Microscopic Description:
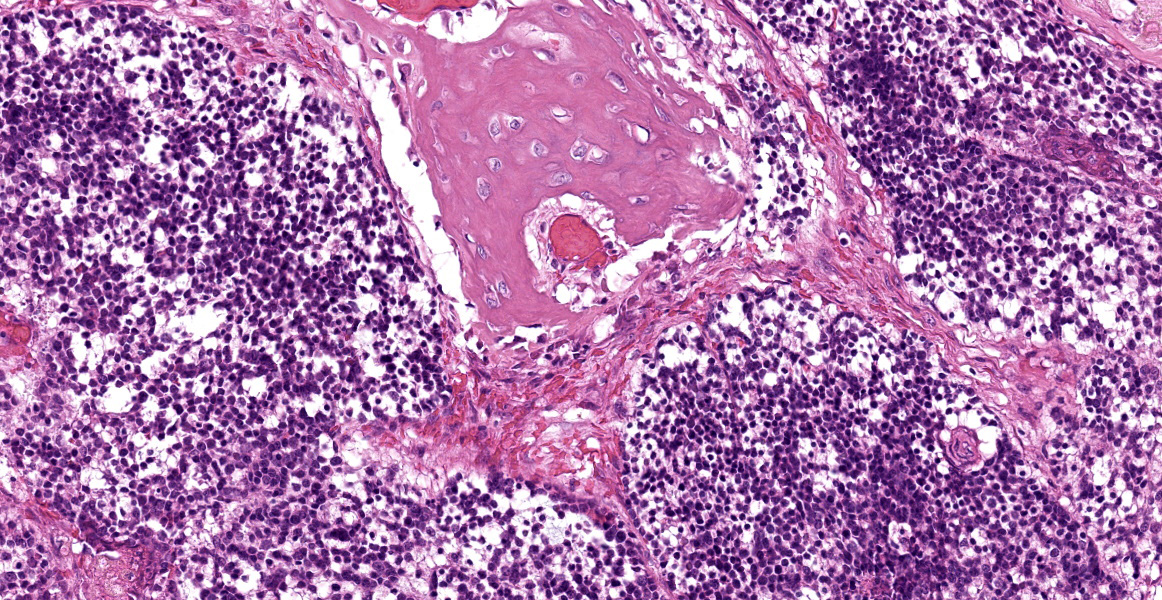
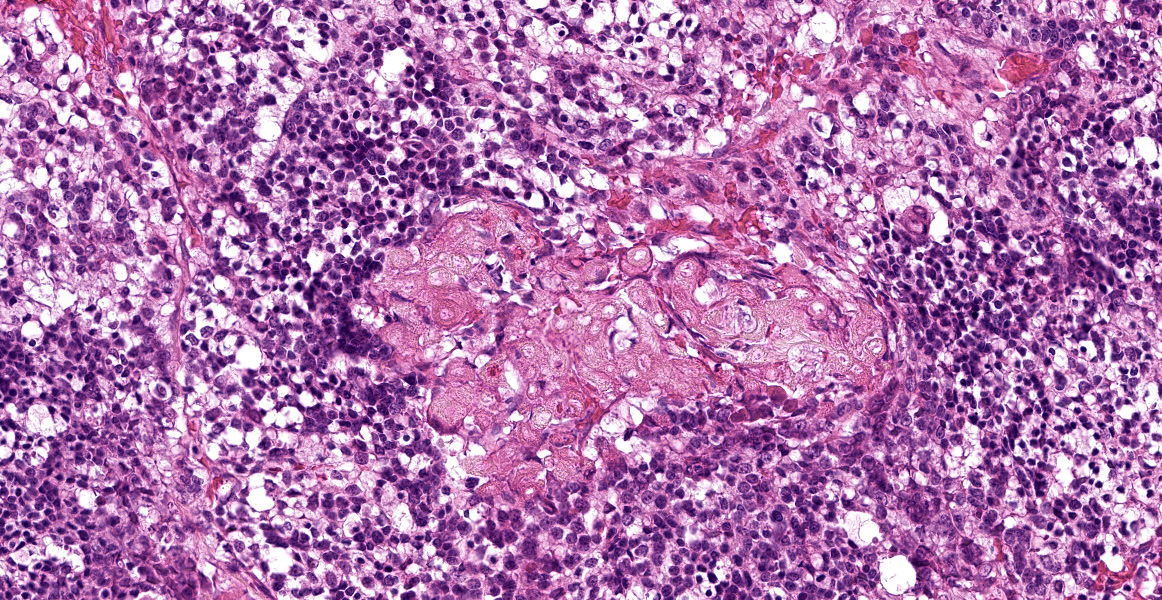
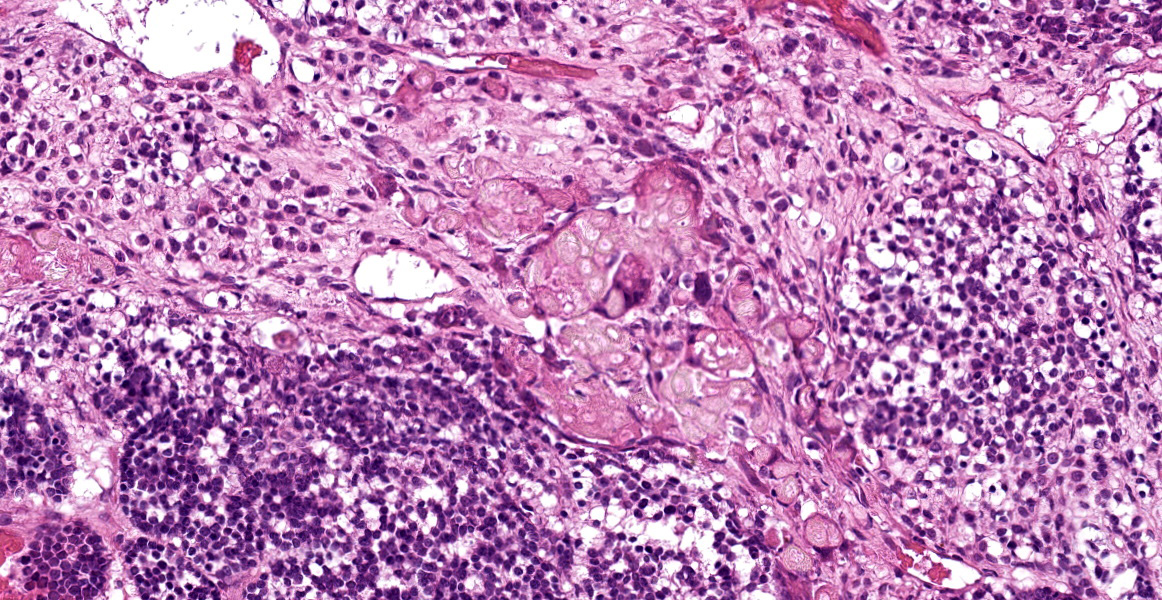
This sample has remnants of normal bone and bony trabeculae of the subchondral/epiphyseal regions. There is a small amount of articular cartilage, some joint space and joint capsule, and opposing bone across and around the joint space. Much of the cortical and trabecular bone is missing and the intertrabecular spaces are filled with sheets of hyperchromatic cells with focal areas of keratin formation. There is some periosteal new bone formation at the edge of the cortical bone and some endosteal new bone formation, but about 90% of this sample is neoplastic tissue. Neoplastic cells form nodules, clusters, and streams of cells that completely fill the intertrabecular spaces. There are some bands of fibrous tissue throughout the lesion. In the centre of nodules and clusters are small hyperchromatic cells similar to those on the periphery and in some, the central cells have more cytoplasm. In many, the cytoplasm is vacuolated. In occasional focal areas there is keratinization with dense keratin and the ghostlike nuclear outline of matricial keratinization. About 10% of this mass is necrotic.
Contributor’s Morphologic Diagnoses:
Metastatic pilomatrixoma to bone with extensive bony lysis and periosteal and endosteal new bone formation.
Contributor’s Comment:
The appearance of the cells within the bone and similar appearing cells in the lung (not
provided) with keratinization of the matricial type is typical of metastasis of pilomatrixoma. It is rare for pilomatrixoma to metastasize, but when they do, previous reports indicate metastasis to the bone is common.
Contributing Institution:
Department of Pathobiology
Ontario Veterinary College
University of Guelph
Guelph, Ontario,Canada
JPC Diagnosis:
Bone: Metastatic pilomatricoma.
JPC Comment:
Pilomatricoma (also known as pilomatrixoma) is an adnexal neoplasm that arises from the germinative cells of the follicular matrix, or hair bulb, and is reported mainly in dogs and humans.1,8 Pilomatricomas are diagnosed most commonly in 4-8 year-old dogs, and Kerry Blue Terriers, Soft Coated Wheaten Terriers, Standard Poodles, and other breeds with continuously growing hair coats are overrepresented in the patient pool, likely because the high number of anagen hair follicles, and their attendant replicating cells, provide fertile soil for neoplastic transformation.1
Consistent with their follicular origin, pilomatricomas typically present as intradermal or subcutaneous masses composed of one or more lobules separated by collagenous stroma.3 The lobules contain a peripheral zone of basophilic cells with hyperchromatic nuclei, a high N:C ratio, and a moderate to high number of mitotic figures.3 The neoplastic cells exhibit an abrupt transition to a central zone of ghost cells which often contain significant accumulations of melanin.3
As the contributor notes, most pilomatricomas exhibit benign, non-metastatic biologic behavior and excision with wide surgical margins is typically curative.3 Malignant pilomatricoma is typically differentiated from its bengin counterpart by being poorly circumscribed, less differentiated, anaplastic, infiltrative, rapidly or erratically growing, and, definitially, metastatic.1,3 Metastatic pilo-matricoma has been reported in various organs, including lymph nodes, lungs, bone, and skin; metastasis to the liver and spleen is less common.1,8 Despite the variety of reported metastatic sites, malignant pilomatricoma seems predisposed to metastasize to bone, with metastasis reported in vertebrae, ribs, the mandible, maxilla, and femur.1
The primary differential for primary or metastatic malignant pilomatricoma is malignant trichoepithelioma, a follicular neoplasm with differentiation to all three segments of the hair follicle.3 Differentiating between these two neoplasms can be difficult, but malignant trichoepitheliomas have tricohyaline granules and prominent inner and outer root sheath differentiation, along with smaller epithelial aggregates, fewer matrical cells, and fewer ghost cells.1,3
The moderator began discussion by noting the palisading layer of cells around the periphery of the neoplastic trabeculae, the first clue that this neoplasm is of epithelial origin. Dr. Craig also noted that the islands of ghost cells can be easily mistaken for necrotic bone with empty lacunae without careful examination. Dr. Craig, a self-described breed predisposition enthusiast, noted that Bassett Hounds are predisposed to pilomatricomas generally and since pilomatricomas often metastasize to bone, metastatic pilomatricoma should be on the differential list for lameness in this breed. As an additional breed-related curiosity, Dr. Craig noted that large breed black dogs, such as the Standard Poodle, Giant Schnauzer, Bouvier des Flanders, and others, unrelated except for size and color, are predisposed to multiple digital squamous cell carcinomas.
The moderator lead a more general discussion of carcinomas within bone, noting that metastatic carcinoma is more common than primary bone tumors in many species. In dogs, metastasis to bone is most frequent in the ribs, vertebrae, and proximal long bones. Dr. Craig noted that most textbooks state that metastasis of carcinomas to bone is uncommon in sites distal to the elbow or stifle; however, there are many examples, including this case, in which metastatic carcinoma is found in more distally, making location an unreliable diagnostic criterion for metastatic carcinoma.
References:
- Carroll EE, Fossey SL, Mangus LM, et al. Malignant pilomatricoma in 3 dogs. Vet Pathol. 2010;47(5):937-43.
- da Silva EO, Green KT, Wasques DG, Chaves RO, dos Reis AC, Bracarense AP. Malignant pilomatricoma in a dog. J Comp Pathol. 2012;147(2-3):214-217.
- Goldschmidt MH, Minday JS, Scruggs JL, Klopfleisch R, Kiupel M. Surgical Pathology of Tumors of Domestic Animals. Vol 1: Epithelial Tumors of Skin. The Davis-Thompson Foundation; 3rd ed:112-114.
- Huzella L, Ide A, Steinbach TJ, Blanchard TW, Lipscomb TP, Schulman FY. Osteosarcoma in malignant pilomatricoma. Vet Pathol 2005;42:700.