Signalment:
Gross Description:
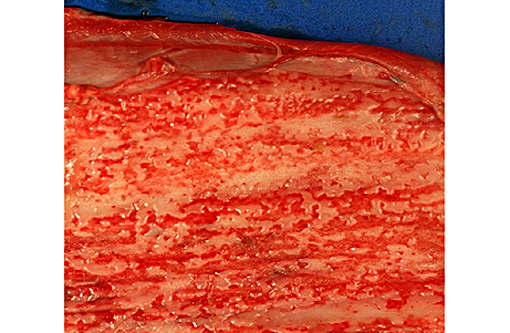
- Multifocal severe ulcerative dermatitis with crusts on muzzle, hooves and one horn
- Multifocal to diffuse exudative dermatitis with skin thickening and matted hairs
- Ulcerative gingivitis and loss of lingual papillae
- Numerous ulcers on esophageal mucosa
- Prescapular lymph node hypertrophy
- Bilateral mucopurulent rhinitis
- Marked congestive laryngitis
Histopathologic Description:
Morphologic Diagnosis:
Lab Results:
Condition:
Contributor Comment:
The pathogenesis, clinical signs and lesions are similar whatever the agent inducing MCF. MCF is characterized by marked T lymphocyte hyperplasia. A population of large granular lymphocytes appears to be infected and transformed by rhadinovirus infection, and OHV-2 genome has been detected in CD8+ T cells. These cells are probably cytotoxic T lymphocytes or T-suppressor cells but the mechanism by which they mediate the lesions of MCF is unclear. Animals probably encounter these viruses through inhalation and ingestion of fomites from oronasal-pharyngeal-ocular fluids from reservoirs animals that are actively shedding virus.(3) Disease is not contagious among affected cattle, which are thought to be dead end hosts. There is a great variation in the presenting clinical syndromes which are potentially pan systemic.(2)
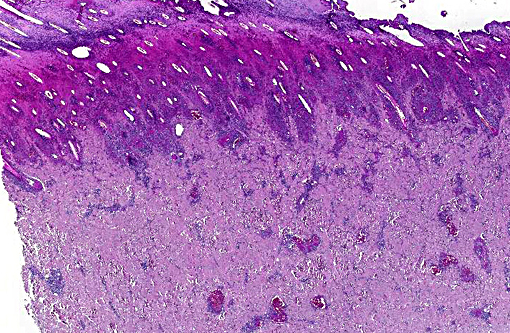
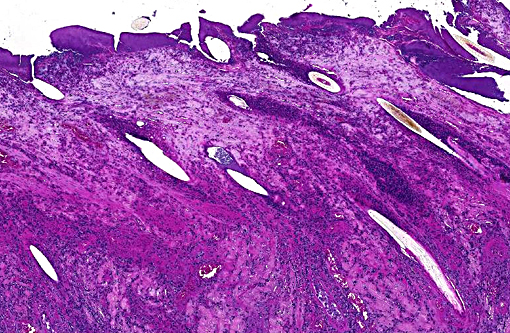
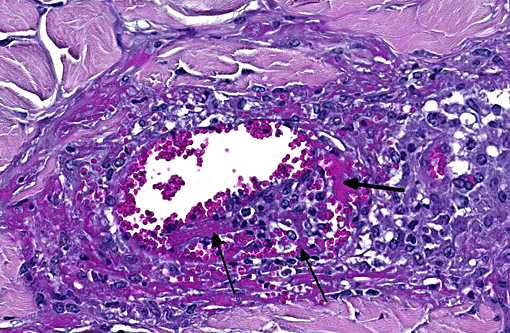
Gross cutaneous lesions especially in sheep-associated MCF are common. Affected areas include the thorax, abdomen inguinal regions, perineum, udder and occasionally the head. Sometimes the cutaneous changes begin in about the base of hooves and horn. In our cases, cutaneous lesions were severe in hooves and coronary band and the cow has lost all epidermal parts of one horn. The characteristic histological changes are found in lymphoid tissue and in the adventitia and walls of medium sized vessels, especially arteries. They are characterized by perivascular accumulation of mainly mononuclear cells and fibrinoid necrotizing vasculitis. These changes may be focal or segmental and may involve the full thickness of the wall or be confined more or less to one layer.
Differentiation of acute severe mucosal disease is sometimes difficult but MCF affects more organs and there is lymphoid hyperplasia whereas lymphoid tissue in BVDV infection is expected to be atrophic. Other differential diagnosis include: bluetongue, vesicular stomatitis, foot and mouth disease, and photosensitization.(3) In our case definitive diagnosis was made by histology and positive OVHV-2 PCR results. This method is sensitive and specific.
Clinical MCF is divided into four variable and overlapping categories:(5)
- Peracute form: Severe oral and nasal mucosal inflammation, hemorrhagic gastroenteritis
- Intestinal form: Pyrexia, diarrhea, hyperemic oral and nasal mucosa with profuse catarrhal and mucopurulent discharge, generalized lymphadenopathy
- Head-and-eye form (most common): Pyrexia, copious serous to mucopurulent ocular and nasal secretions, encrusted muzzle with occluded nostrils, dyspnea and open-mouthed breathing, oral mucosal hyperemia with erosions, sloughed buccal mucosal tips; Ocular lesions: Ophthalmia, photophobia, palpebral conjunctival hyperemia and edema, corneal opacity, +/- hypopyon
- Mild form: mild oral and nasal mucosal erosions
JPC Diagnosis:
Conference Comment:
OVHV-2 can be a contentiously complicating infectious disease for producers, as owners of sheep can move flocks in and out of a facility without consequence while an adjacent closed-herd of cattle or bison suffers severe outbreaks. In endemic areas, nearly all sheep are infected during their first year of life and rarely develop clinical disease; which is in stark contrast to infection in cattle where the clinical course typically ends in death or euthanasia. Even in cases where outbreaks of systemic vasculitis occur in a sheep flock and positive detection of viral antigen is confirmed, OVHV-2 can only be considered with suspicion. The detection of ORF25, a viral-encoded protein of OVHV-2, would be more persuasive in such instances.(3)
All gammaherpesviruses have a tropism for T or B lymphocytes, and members of the MCF viruses preferentially target T cells.(3) Infected CD8+ T lymphocytes spread the virus systemically and incite production and recruitment of proinflammatory cytokines which lead to the tremendous lesions observed.(4) In sheep, only aerosol challenges result in infection, where initial replication occurs within type II pneumocytes. Intravenous, intraperitoneal, and transplacental inoculations do not result in infection while infected colostrums may rarely result in infection.(3)
The contributor mentioned important differentials to consider in cases which present with acute mucosal disease. The endemicity of MCF, BVDV, and now bluetongue among cattle in Europe make obtaining a definitive diagnosis of special importance. Studies have characterized MCF and BVDV as being more clinically similar; however, cattle with bluetongue more often have a better appetite, demeanor and facial appearance and do not have bilateral lymph node enlargement.(1)
References:
1. Bexiga R, Guyot H, Saegerman C, et. al. Clinical differentiation of malignant catarrhal fever, mucosal disease and bluetongue. Vet Rec. 2007;161:858-859.Â
2. Brown CC, Baker DC and Barker IK. Alimentary system. In: Maxie MG, ed. Jubb, Kennedy and Palmers Pathology of Domestic Animals. Vol 2. 5th ed. Philadelphia, PA: Elsevier Saunders; 2007:152-158
3. D. OToole and H. Li: the pathology of malignant catarrhal fever with an emphasis on Ovine Herpesvirus 2. Veterinary Pathology 51(2) :437-452, 2014
4. James F. Zachary Mechanisms of microbial infections in pathologic basis of disease fifth edition 2012, p219
5. Joint pathology VSPO U-V02 - Malignant catarrhal fever (MCF) - kidney, haired skin - steer