Signalment:
- The kennel has a 10-11 month history of infertility.
- Three stud dogs and 11 bitches.
- No litters from March until Jan 27, 2008. (One puppy born to a previously negative bitch was bred to a positive male in Nov. Her most recent B. canis test at Cornell for AGID month #2 in kennel eradication.) Tested 14 dogs, Jan 4, 2008, 8 of 14 positive at Cornell by AGID.
- Euthanized 5 dogs Jan 30, 2008
- Spayed and neutered 2 dogs on Feb 1, 2008 and started on Doxycycline (28 days) and Gentamicin (7 days) unless culture and sensitivity reveal better options.
Infertility. Small soft testicles with firm epididymis bilateral. Left testicle had a fluid filled lesion on ultrasound. Prostate enlarged, fluctuant and painful, straining to defecate and blood in stool. Mild conjunctivitis.
Gross Description:
Histopathologic Description:
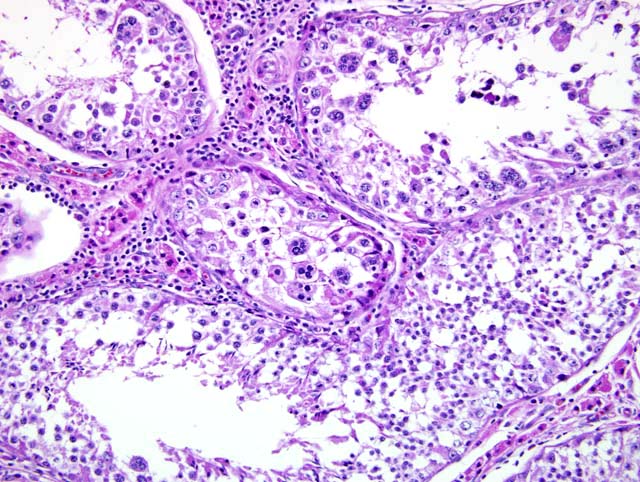
Testicles: There is diffuse, severe atrophy of the seminiferous tubules. In several areas, there are small clusters of remaining tubules that are small, hypocellular and have thickened hyalinized basement membranes. There is no evidence of spermatogenesis. Conspicuous clusters of interstitial cells are present within the testicle. There is diffuse lymphohistiocytic infiltration throughout the parenchyma. In addition, there is one cavity containing ischemic necrotic tissue sequestrum surrounded by dense lymphohistiocytic infiltrates.Â
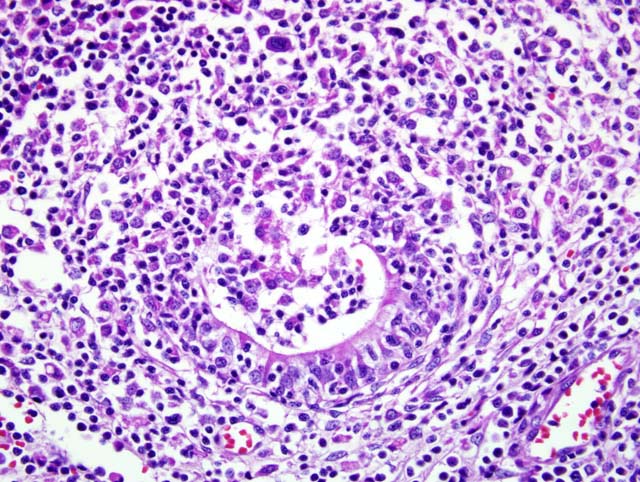
Epididymis: The lesions are similar to those in the testicle with diffuse, dense sheets of lymphohistiocytic cells, atrophic tubules, inflammatory cell infiltrates in tubular walls, plus intense lymphohistiocytic clusters within tubules (Fig. 3-1). There are no spermatids in epididymal tubules.Â
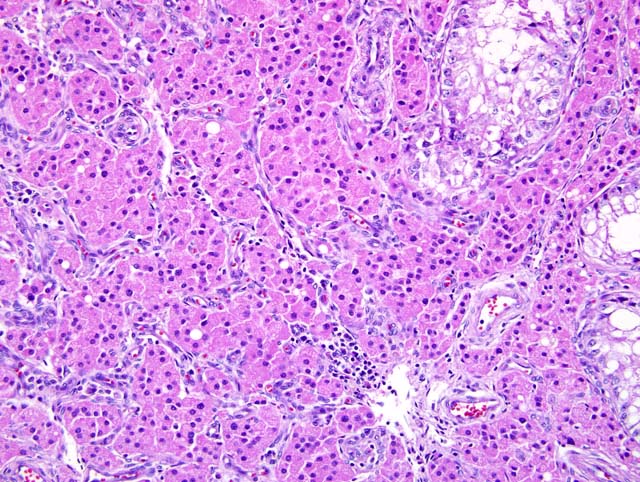
Prostate gland: The majority of the prostate gland examined is composed of hyperplastic acini lined with a single layer of tall, plump columnar epithelium with abundant eosinophilic cytoplasm. An occasional small lymphoid nodule is present within the interstitium of these areas. Within one lobe, there is marked acinar atrophy with reduction in the number of acini and diffuse, dense sheets of lymphocytes, plasma cells and macrophages. The remaining acinar walls are moderately infiltrated with primarily lymphocytes.Â
*** Sections submitted will contain either testicle, testicle and epididymis, or prostate gland.
Morphologic Diagnosis:
Testicles: Orchitis, lymphohistiocytic, chronic, severe, diffuse with marked seminiferous tubular atrophy and focal necrosis (Fig. 3-2)
Epididymis: Epididymitis, lymphohistiocytic, chronic, severe
Lab Results:
Condition:
Contributor Comment:
Brucellosis in dogs has been described with B. melitensis, B. suis, B. abortus and B. canis; however, only B. canis is considered epidemiologically significant.(4) B. canis has been reportedly recovered from just about every bodily fluid and/or surface: vaginal secretions, semen, abortuses, milk, urine, saliva, ocular secretions and feces.(4) The organism is transmitted through venereal and/or oral routes. Following entry, the organism is taken up by the mononuclear-phagocytic system and distributed to the lymphoid and genital compartment where the organisms multiply.(4) Bacteremia develops and proliferation of the organism in the target organs results in the lesions typical of the disease: uterine infection and abortion in females, epididymitis and prostatitis in males, lymphadenitis, discospondylitis, anterior uveitis, dermatitis, meningoencephalitis (refer to nice flow chart, pg. 197 of Ref. #4). Diagnosis is achieved through serology, agglutination tests, agar gel immunodiffusion, ELISA, and immunofluorescence; however, definitive diagnosis can only be made through retrieval of the organism from bacterial culture.(4) Treatment is difficult, in part because of the intracellular nature of the organism. Many different drugs and drug combinations have been tried, but no combination has been found to be 100% effective.(4) Combination drug treatments have shown better efficacy than single antibiotic therapies.(4) Lastly, B. canis has zoonotic potential. The incidence of human infections is not known.(4) People contract the disease through contact with the organism shed during abortions or in research laboratories where people work directly with the organism.(4)
JPC Diagnosis:
1. Testicle: Orchitis, lymphohistiocytic, chronic, diffuse, severe, with marked seminiferous tubular atrophy and loss, and interstitial cell hyperplasia
2. Epididymis: Epididymitis, lymphohistiocytic, chronic, diffuse, severe
3. Epididymis: Epithelial hyperplasia, diffuse, marked
Conference Comment:
Abortions caused by B. canis are normally late gestational abortions that occur after 50 days. As seen in this case, the usual sequelae to B. canis infection in male dogs is epididymitis and testicular degeneration. This often causes severe scrotal irritation and affected dogs often focus on this discomfort and lick the area until it is ulcerated. Lymphadenopathy of the mandibular and retropharyngeal lymph nodes is common. Placental lesions consist of necrosis of chorionic villi with a plethora of bacteria within infected trophoblastic cells. Infected females often discharge copious amounts of foul vaginal secretions after abortion, which is an excellent means of disease transmission. Fetal lesions are fatal and include pneumonia, endocarditis, and hepatitis.(2)
Brucella canis is caused by a mucoid strain of Brucella that is similar to Brucella suis. Because of its mucoid nature, B. canis lacks surface antigens that B. abortus and B. melitensis have, thus rendering conventional test methods ineffective.(2)
References:
2. Schlafer DH, Miller RB: Female genital system. In: Jubb, Kennedy, and Palmer's Pathology of Domestic Animals, ed. Maxie MG, vol. 3, pp. 484-489. Elsevier Limited, Philadelphia, PA, 2007
3. Schoeb TR, Morton B: Scrotal and testicular changes in canine brucellosis: a case report. J Am Vet Med Assoc. 172:598-600, 1978
4. Wanke, MM: Canine brucellosis. Anim Reprod Sci. 82-83:195-207, 2004