Signalment:
Gross Description:
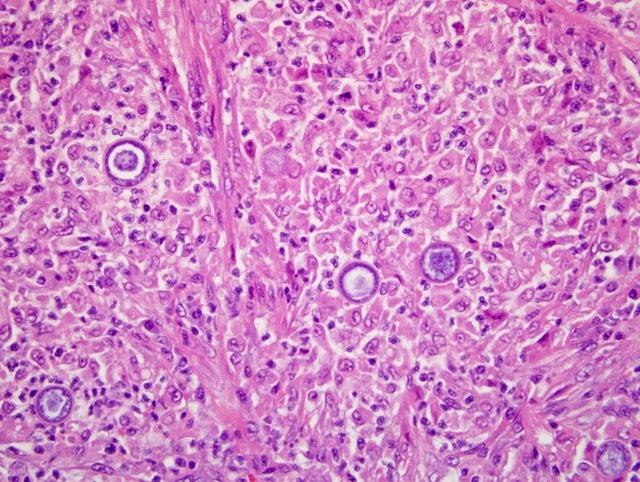
Histopathologic Description:
Morphologic Diagnosis:
Condition:
Contributor Comment:
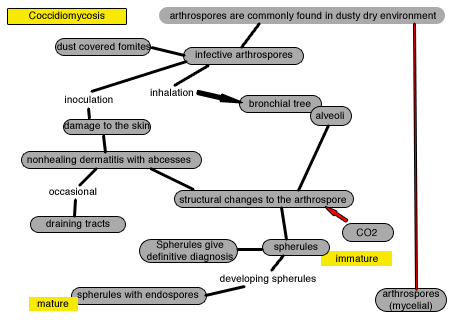
The disease is also known as San Joaquin Valley Fever (in California), Desert fever, and Valley Fever. It is an endemic disease in specific ecological regions that include the southern United States, northern parts of Mexico and some countries in South America. Coccidioidomycosis is a dimorphic fungus; in soil it presents as a mycelium or arthrospore form that behaves as a saprophytic organism, and when the fungus gains access to tissues and body fluids it becomes the spherule form where it behaves as a parasitic organism. The pathogenesis starts with inhalation of the infective arthrospores (common in dry environment especially after a long dry weather season followed by heavy rain) or direct inoculation to the skin.
Even though the disease affects humans it is not considered a zoonosis. This disease is not transmitted through animal-animal contact. The only mode of transmission is through contaminated soil or dust with mature arthrospores. Coccidioidomycosis could develop infective arthrospores during fungal culture and laboratory workers should be cautioned for possible source of infection.
Cats are not particularly susceptible to coccidioidomycosis compared to dogs. The most common presentation in cats is skin and pulmonary. Clinical signs are not very specific, as this organism can affect different tissues including skin, lung, eyes, nervous tissue.
Diagnostic tests available include:
1. Cytology smears/ FNA with identification of spherules (definitive diagnosis)
2. Histopathology with identification of spherules (definitive diagnosis). The variable morphology of C immitis is diagnostic: Sporangia 30-200 um in diameter containing 2-4 um endospores (mature spherules); immature spherules
3. Agar gel immunodeficiency (AGID) assay for IgG and IgM- specific test but not sensitive enough
4. ELISA to detect IgG and IgM- sensitive test but false positive results are common. Serological tests appear to be poor in cats
Greene described 48 feline coccidioicomycosis cases with skin (56%), respiratory (25%) musculoskeletal (19%), and CNS and ophthalmic (19%) involvement. There is no current effective treatment available. Fungal culture is not a useful diagnostic tool since definitive identification depends on spherule formation which is the only form in tissues during the parasitic phase of the life cycle of this peculiar fungus. Species affected by this fungus include many mammalian species such as dogs, cats, horses, sheep, cattle, pigs, non-human primates and South American camelids.
The OIE reports this disease as a differential for tuberculosis since the granulomatous, multifocal to coalescing inflammatory process will efface the normal architecture in lymph nodes and lung similar to the pattern encountered in tuberculosis.
JPC Diagnosis:
Conference Comment:
Conference participants discussed the typical clinical presentation of Coccidioides immitis infection in the dog and cat. Most infections in the dog are pulmonary, with occasional systemic dissemination to multiple organs including bones and the skin. Bone infections tend to occur in long bones, and result in both lytic and productive lesions; thus, radiographically, coccidioidal osteomyelitis is included in the differential diagnosis for osteosarcoma. In contrast to dogs, the lesions in cats are primarily cutaneous and clinically characterized by multiple draining nodules without underlying bone involvement.
The moderator shared some experiential histopathologic features of pulmonary blastomycosis, coccidioidomycosis, and cryptococcosis. In general, pulmonary blastomycosis tends to be fibrosing; coccidioidomycosis is necrotizing; and cryptococcosis incites very little inflammatory response.
Conference participants also briefly reviewed some of the microorganisms which reproduce via endosporulation, including :
- Coccidioides immitis
- Rhinosporidium seeberi
- Prototheca wickerhamii, P. zopfi
- Chlorella spp.
- Batrachochytrium dendrobatidis (chytridiomycosis)
References:
2. Chandler FW, Watts JC. Coccidioidomycosis. In: Pathologic Diagnosis of Fungal Infections. Chicago, IL: ASCP Press; 1987:13-15.
3. Chiller TM, Galgiani JN, Stevens DA. Coccidioidomycosis. Infect Dis Clin N Am. 2003;17:41-57.
4. Graupmann-Kuzma A, Valentine BA, Shubitz LF, Dial SM, Watrous B, Tornquist SJ. Coccidioidomycosis in dogs and cats: a review. J Am Anim Hosp Assoc. 2008;44:226-235.
5. Greene RT, Troy GC. Coccidioidomycosis in 48 cats: a retrospective study (1984-1993). J Vet Intern Med. 1995;9:86-91.
6. Greene RT. Coccidioidomycosis. In: Greene CE, ed. Infectious Diseases of Dogs and Cats. 2nd ed. Philadelphia, PA: WB Saunders Co.; 2002:391-398.
7. Kerl ME. Update on canine and feline fungal diseases. Vet Clin North Am. 2003;33:721-747.
8. Kumar V, Abbas AK, Fausto N, Aster JC. Acute and chronic inflammation. In: Kumar V, Abbas AK, Fausto N, Aster JC eds. Robbins and Cotran Pathologic Basis of Disease. 8th ed. Philadelphia, PA: Elsevier Saunders; 2009:73-74.
9. OIE, Center for food Security and Public Health: Coccidioidomycosis. http://www.cfsph.iastate.edu/Factsheets/pdfs/coccidioidomycosis.pdf CVM, Iowa State University, Ames, IA, 2004