Signalment:
- Dyspnea - RR 40 bpm - Increased bronchovesicular sounds
- HR 132 bpm, no murmur at this time
- Vulvar mucosa gray-pink
- Lethargy, Weakness, Anorexia
- Patient = 74 mmHg Systolic, 42 mmHg Diastolic (Pulmonary hypertension)
- Normal = 20 to 25 mmHg, 8 to 10 mmHg
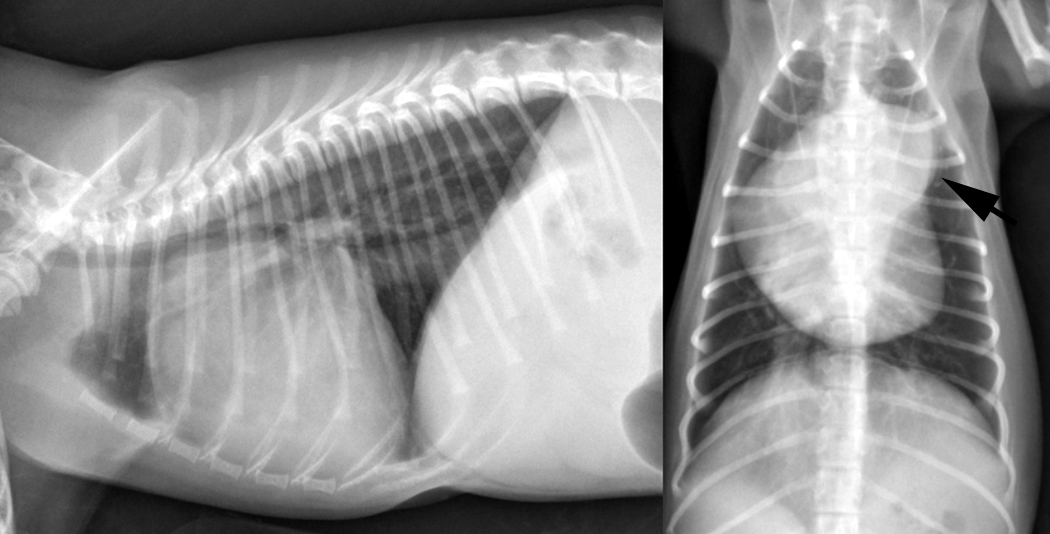
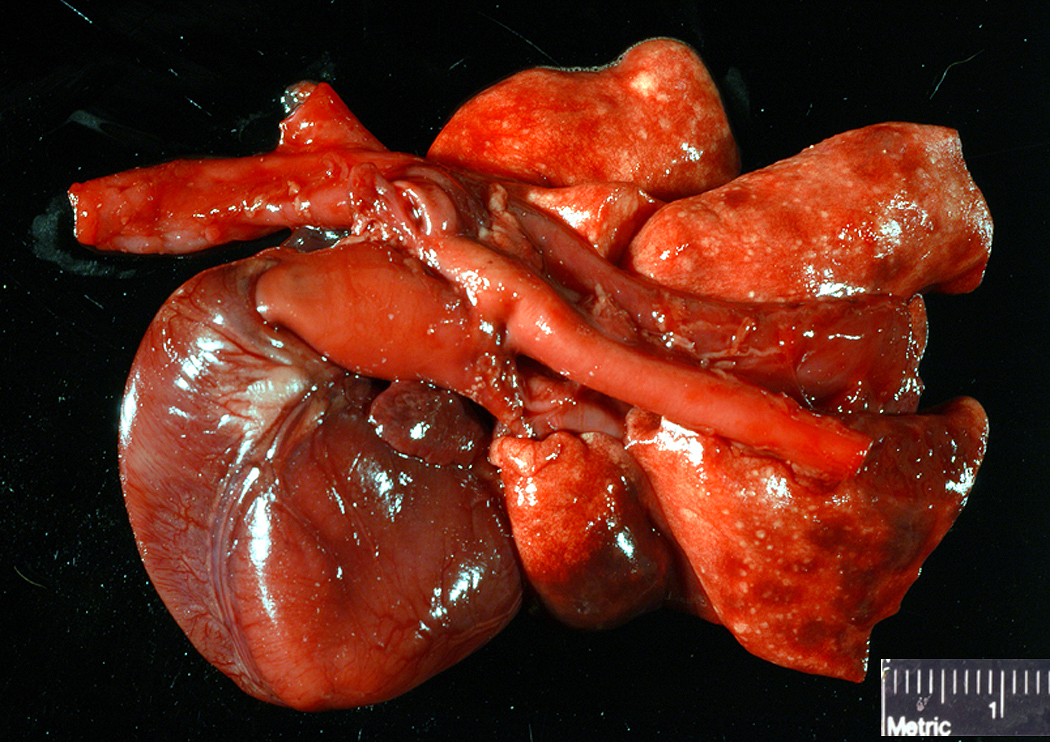
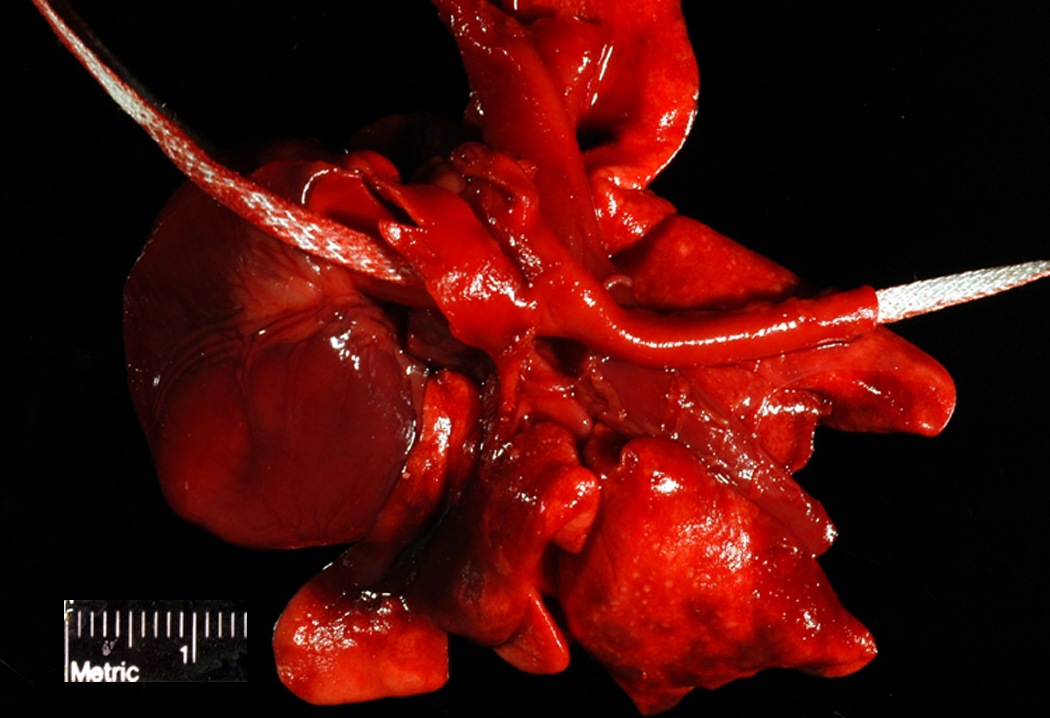
- Severely dilated RA and RV
- Severely dilated proximal pulmonary artery
- Decreased LV and LA filling
Patient was euthanized after developing apnea and bradycardia. Necropsy was delayed due to scintigraphy study, resulting in some autolysis. Owners requested cosmetic exam restricted to thorax.
Gross Description:
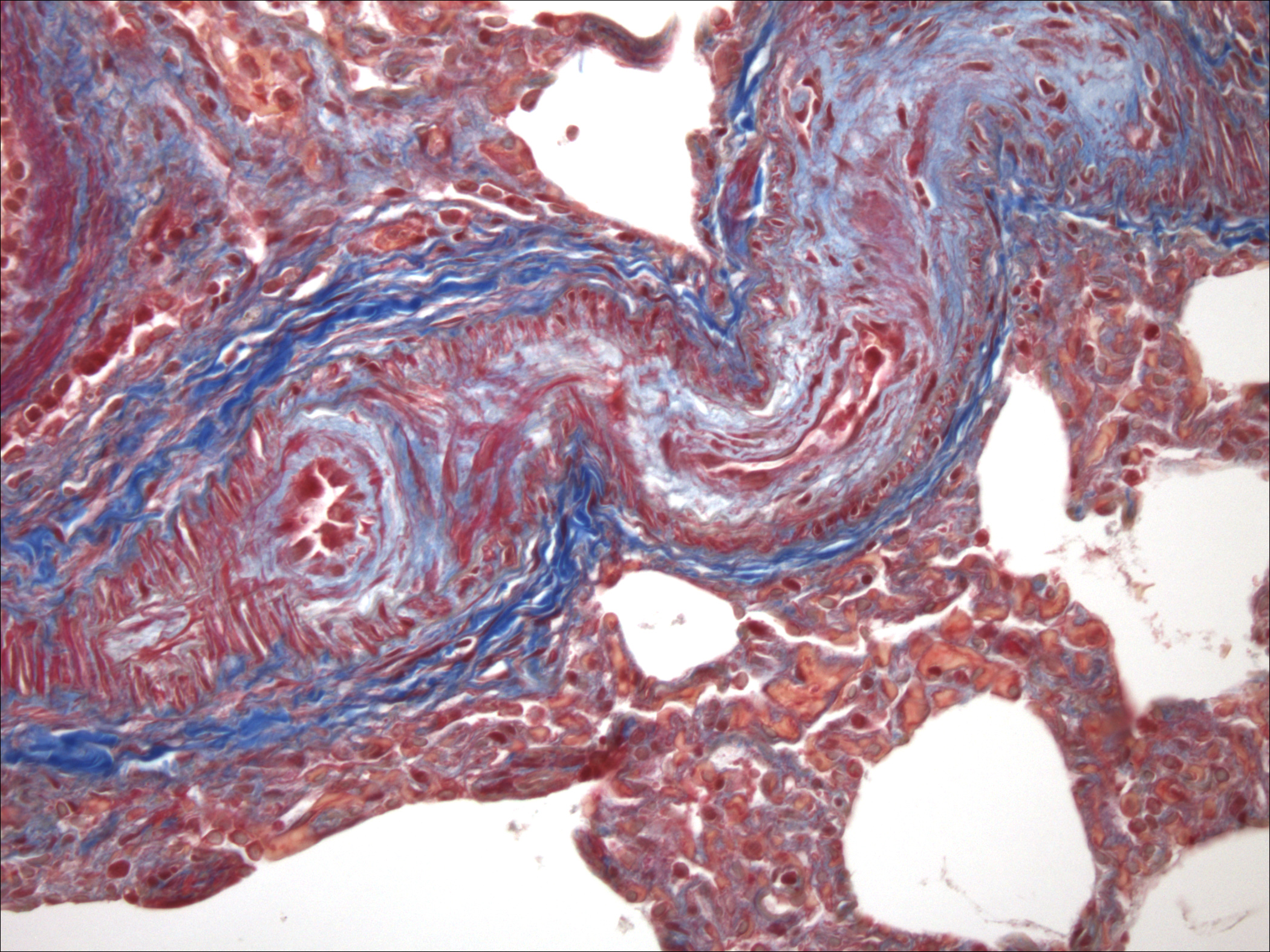
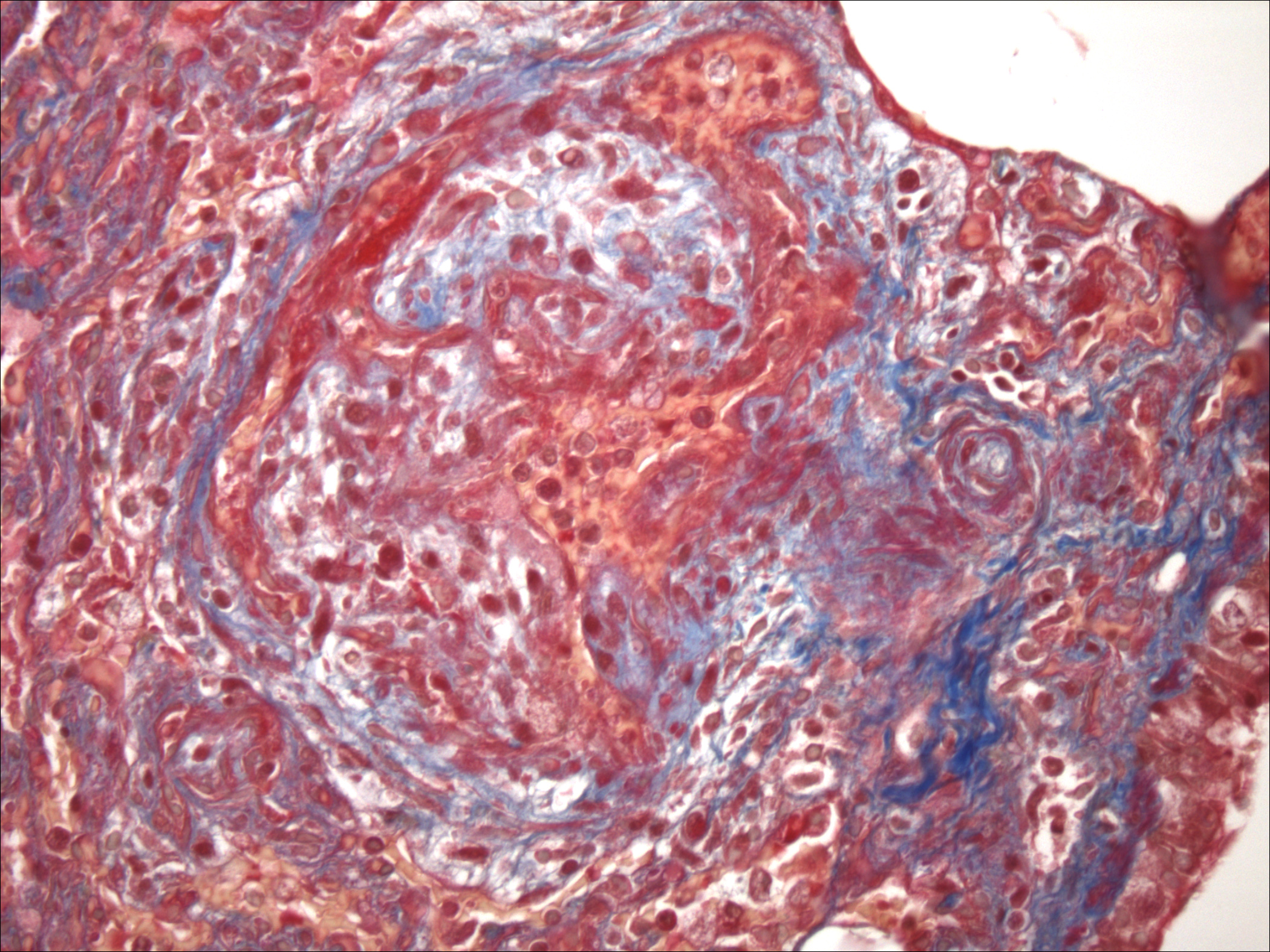
Histopathologic Description:
Morphologic Diagnosis:
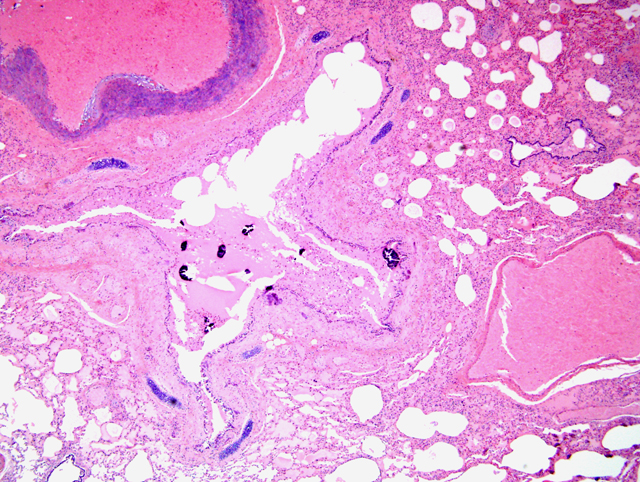
2. Mild multifocal alveolar fibrosis and emphysema
3. Moderate multifocal bronchial and alveolar mineralization
Lab Results:
Condition:
Contributor Comment:
1. The pulmonary vasculature does not respond (dilate) as it should at birth, with inflation of the lung, and the prenatal pressure gradient from right heart to left is maintained after birth.Â
2. After birth the normal shift in pressure gradient occurs across the ductus and shunting of blood across the PDA from the left to right outflow tracts results in increased circulation through the pulmonary vasculature. Eventually this over-circulation induces arterial sclerosis, hypertension and reversal of the gradient across the ductus from right to left.
While either scenario is possible with this clinical presentation, the histologic arterial changes and pulmonary arterial pressures, as per analysis of echocardiograms, are more consistent with the latter. The vascular lesions in the lung are most consistent with a reactive change and would also exacerbate the progression of hypertension over time. The distinct murmur detected at 3 months of age and absent 2 months later, just before euthanasia, likely reflects this dynamic process as hypertension developed and resulted in changes in blood flow through the ductus.Â
The etiology of pulmonary mineralization is most likely related to azotemia. Urinalysis suggested significant tubular damage but BUN and creatinine values were not available and kidneys were not examined because necropsy was restricted to the thorax.Â
JPC Diagnosis:
2. Lung: Mineralization, interstitial, vascular, multifocal.
3. Lung: Edema, multifocal, moderate.Â
Conference Comment:
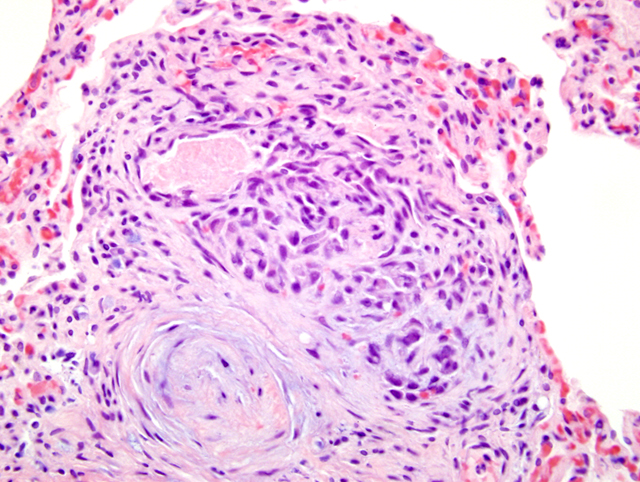
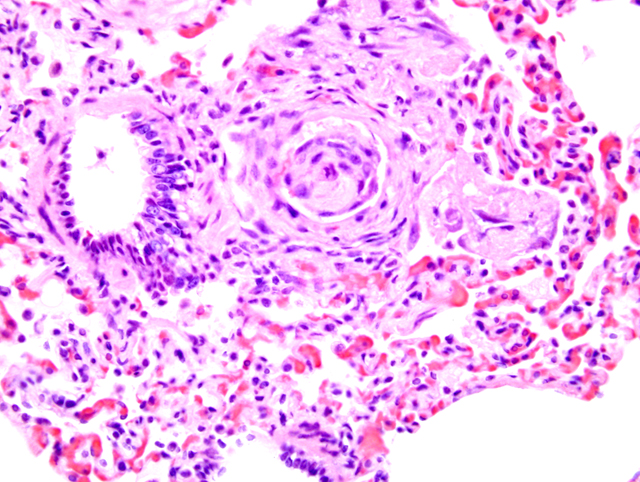
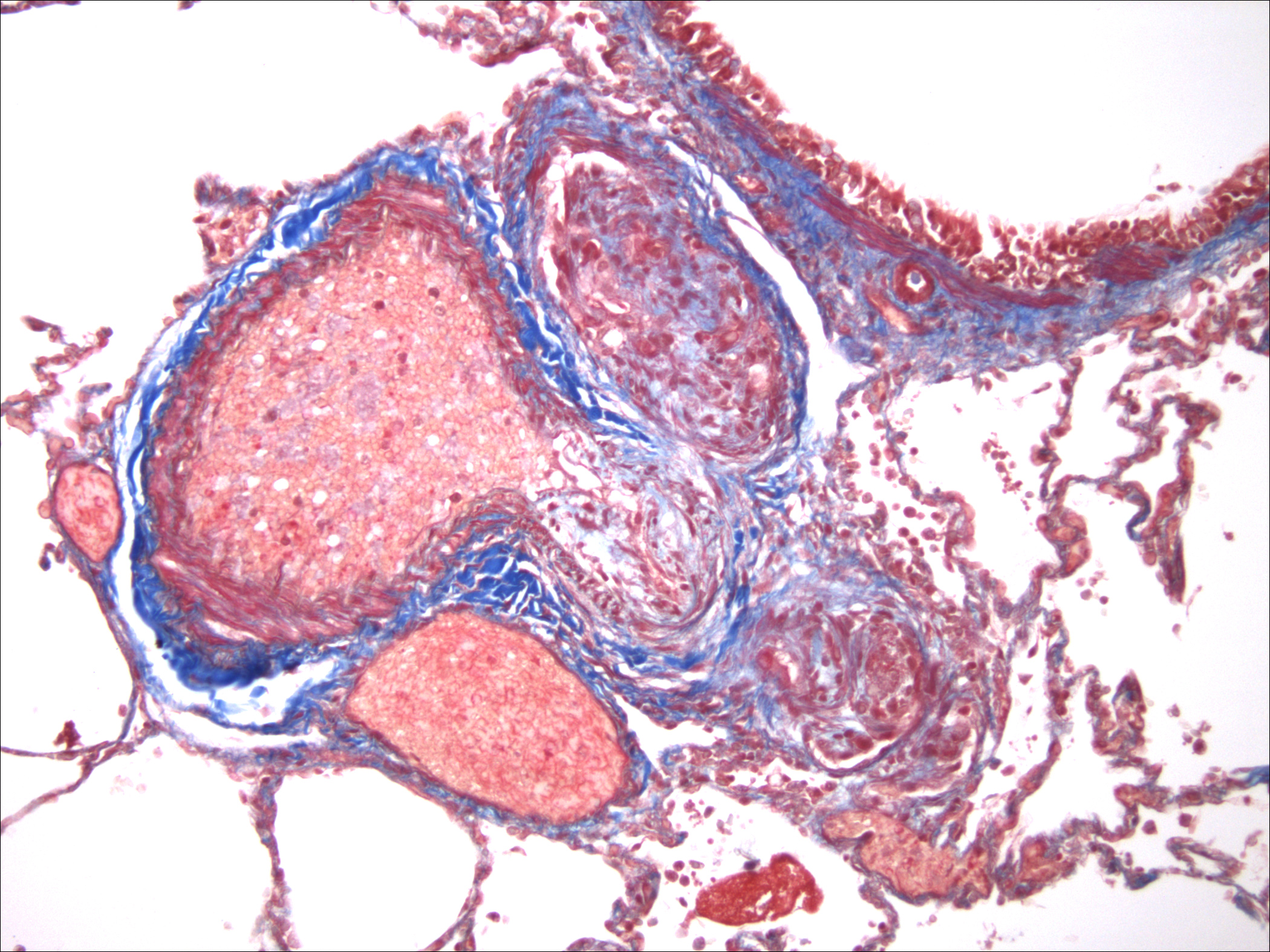
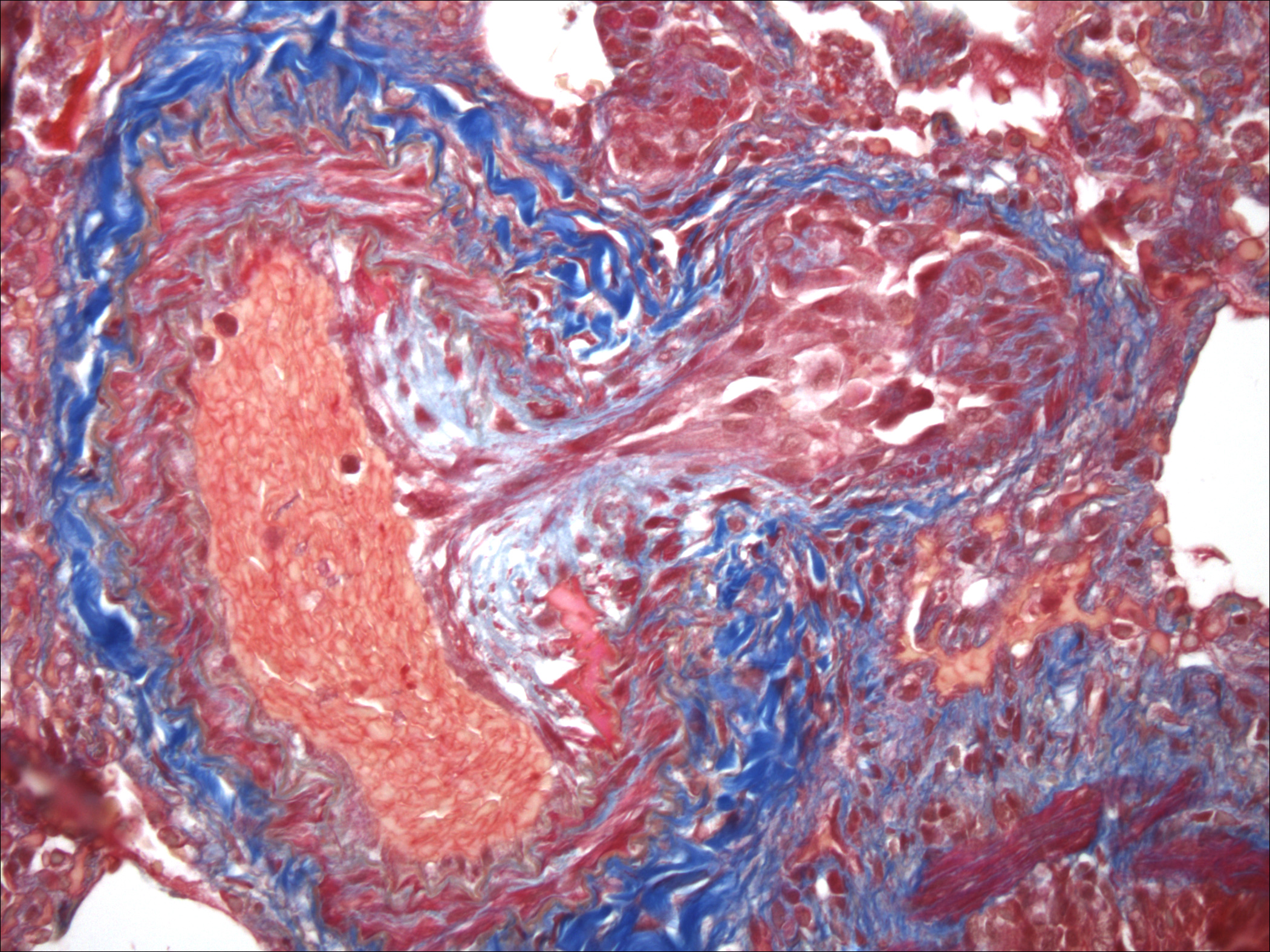
Pulmonary arteriopathy (plexogenic pulmonary arteriopathy) is a condition characterized by constrictive and complex, obstructive, and proliferative vascular lesions in the pre- and intra-acinar pulmonary arteries that results in pulmonary arterial hypertension and eventually right-sided heart failure.20 Pulmonary arterial hypertension with pulmonary arteriopathy can be subdivided into idiopathic, familial and associated with risk factors or conditions. Most cases in dogs have been idiopathic or associated with congenital heart disease, particularly patent ductus arteriosus.9,16 Histologic lesions include plexiform lesions of the small arterioles with concentric intimal cellular proliferation and fibrosis, non-specific medial hypertrophy, muscularization of arterioles, fibrinoid degeneration and arteritis.1,2,7,9,15,16 The association between pulmonary hypertension and the development of pulmonary arteriopathy is not fully understood as each may contribute to the formation of the other.
The pathogenesis of the changes within the small and medium sized pulmonary arteries seen in cases of pulmonary hypertension is not clear. Potential factors associated with this condition may be due to a genetically based hyperreactivity of pulmonary arteries18, sheer stresses on the pulmonary arteries, injury to the pulmonary endothelium, or changes induced by toxins, drugs and infections.6,11,14,19 Chronic changes within the pulmonary arteries due to increased flow have been associated with altered nitric oxide and endothelin respones.4 Endothelin-1, a potent vasoconstrictor, has been associated with increased pulmonary flow in left-to-right shunts independent of pulmonary artery pressure.4,17 Pulmonary arteries exposed to high flow and pressure also have been reported to have increased levels of VEGF, which suggests the ongoing process of tissue remodeling.10,12
References:
2. Buchanan, JW: Patent ductus arteriosis morphology, pathogenesis, types and treatment. J Vet Cardiol 3:7-16, 2001
3. Fishman AP: Pulmonary hypertension. In: Hurst's The Heart, eds. Alexander RW, Schlant RC, Fuster V, 9th ed., pp. 1699-1717. McGraw-Hill, New York, NY, 1998
4. Gavaghan BJ, Lapointe JM, Thomas WP: Acute onset of pulmonary necrotising arteritis in a dog with a left-to-right patent ductus arteriosus. Aust Vet J 76:786-791, 1998
5. Glaus TM, Hauser K, Hassig M, Lipp B, Reusch CE: Non-invasive measurement of the cardiovascular effects of chronic hypoxaemia on dogs living at moderately high altitude. Vet Rec 152:800-803, 2003
6. Glaus TM, Soldati G, Maurer R, Ehrensperger F: Clinical and pathological characterisation of primary pulmonary hypertension in a dog. Vet Rec 154:786-789, 2004
7. Heath D, Edwards J: The pathology of hypertensive pulmonary vascular disease: a description of six grades of structural changes in the pulmonary arteries with special reference to congenital cardiac septal defects. Circulation 18:533-547, 1958
8. Johnson L, Boon J, Orton EC: Clinical characteristics of 53 dogs with Doppler-derived evidence of pulmonary hypertension: 1992-1996. J Vet Intern Med 13:440-447, 1999
9. . Kolm US, Amberger CN, Boujon CE, Lombard CW: Plexogenic pulmonary arteriopathy in a Pembroke Welsh corgi. J Sm Anim Pract 45:461-466, 2004
10. Lam CF, Peterson TE, Croatt AJ, Nath KA, Katusie ZS: Functional adaptation and remodeling of pulmonary artery in flow-induced pulmonary hypertension. Am J Physiol Heart Circ Physiol 289:H2334-H2341, 2005
11. Lee S, Shroyer KR, Markham NE, Cool CD, Voelkel NF, Tuder RM: Monoclonal endothelial cell proliferation is present in primary but not secondary pulmonary hypertension. J Clin Invest 101:927-934, 1998
12. Mata-Greenwood E, Meyrick B, Soifer SJ, Fineman JR, Black SM: Expression of VEGF and its receptors Flt-1 and Flk-1/KDR is altered in lambs with increased pulmonary blood flow and pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol 285:L222-L231, 2003
13. Perry LA, Dillon AR, Bowers TL: Pulmonary hypertension. Comp Cont Educ Pract 13:226-232, 1991
14, Rubin LJ: Primary pulmonary hypertension. N Engl J Med 336:111-117, 1997
15. Tuder RM, Groves B, BAdesch DB, Voelkel NF: Exuberant endothelial cell growth and elements of inflammation are present in plexiform lesions of pulmonary hypertension. Am J Pathol 144:275-285, 1994
16. Turk JR, Miller JB, Sande RD: Plexogenic pulmonary arteriopathy in a dog with ventricular septal defect and pulmonary hypertension. J Am Anim Hosp Assoc 18:608-612, 1982
17. Vincent JA, Ross RD, Kassab J, Hsu JM, Pinsky WW: Relation of elevated plasma endothelin in congenital heart disease to increased pulmonary blood flow. Am J Cardiol 71:1204-1207, 1993
18. Wagenvoort CA: Open lung biopsies in congenital heart diseases for evaluation of pulmonary vascular disease: predictive value with regard to corrective operability. Histopathol 9:417-436, 1985
19. Yeager ME, Halley GR, Golpon HA, Voelkel NF Tuder RM: Microsatellite instability of endothelial cell growth and apoptosis genes within plexiform lesions in primary pulmonary hypertension. Circ Res 88:e2-e11, 2001
20. Zabka TS, Campbell FE, Wilson DW: Pulmonary arteriopathy and idiopathic pulmonary arterial hypertension in six dogs. Vet Pathol 43:510-522, 2006