Joint Pathology Center
Veterinary Pathology Services
Wednesday Slide Conference
2019-2020
Conference 8
23 October 2019
Dr. Dalen Agnew, DVM,
PhD, DACVP
Associate Professor
Pathobiology and Diagnostic Investigation
Michigan State University
College of Veterinary Medicine
East Lansing, Michigan
CASE IV: TAMU 2017 WSC 2 (JPC 4102428).
Signalment: 7-year-old, American Quarter Horse mare, Equus ferus caballus
History: Four weeks prior to presentation at the end of April, this working Quarter Horse mare had had a tooth extraction under anesthesia. Approximately 2 weeks prior to presentation, the horse became dyspneic with a nasal discharge and coughing. She was treated with Uniprim (trimethoprim and sulfadiazine) without resolution, and at 5 days before presentation, her treatment was switched to doxycycline, banamine and Previcox (NSAID's Cox-2 inhibitor). Because the dyspnea worsened, she was taken to a veterinarian, and she was found to be febrile (103.6F) and severely dyspneic. She was referred to TAMU, and at presentation, the mare continued febrile, and dyspneic with a bilateral nasal discharge. Ultra sound showed bilateral consolidation with a flocculent, pleural effusion especially on the right where a hypoechoic fluid pocket at the level between ribs 9-15 in which gas was trapped was noted.
The chest drains were lavaged daily, and the mare receive LRS fluids, antibiotics (gentamicin then chloramphenicol) and antiinflammatories; however, the lesion and signs progressed, and she was euthanized after 3 days of hospitalization
Gross Pathology: A 422 kg (929 lb) seven-year-old, red roan, Quarter Horse mare with a white sock on the right hind and in adequate body condition is necropsied on April 27, 2017.
INTEGUMENTARY/SPECIAL SENSES: Shaved areas include: 10x10cm on the right mid thorax and 10x10 cm on the right side of the mid-cervical neck. A 3 cm, linear, superficial abrasion is caudal to the right eye.
RESPIRATORY: Approximately 5 L of yellow to grey, turbid fluid are in the pleural cavity, and a large amount of yellow, friable material is admixed with the fluid and firmly adhered to the lung (fibrinopurulent pleuritis). Diffusely, the costal and diaphragmatic pleura are dark red and markedly thickened (reactive mesothelium). The ventral lungs are diffusely firm and dark red (bronchopneumonia). In the middle of the right lung is a focal, 10x10x15 cm cavitation that connects to bronchi and contains a large amount of tan, casts of grey red, moist, friable material (Aspiration Pneumonia with sequestrum formation).
CARDIOVASCULAR (Heart weight: 4.19 kg; Right ventricular wall: 1 cm; Left ventricular wall: 3 cm): The pericardium is markedly and irregularly thickened and dark red (reactive mesothelium). The right side of the heart is mildly thickened (hypertrophy, pulmonary hypertension).
ENDOCRINE: A 1.5x0.5 cm, raised, pink to grey, mass is in the pituitary gland (pituitary adenoma, presumed).
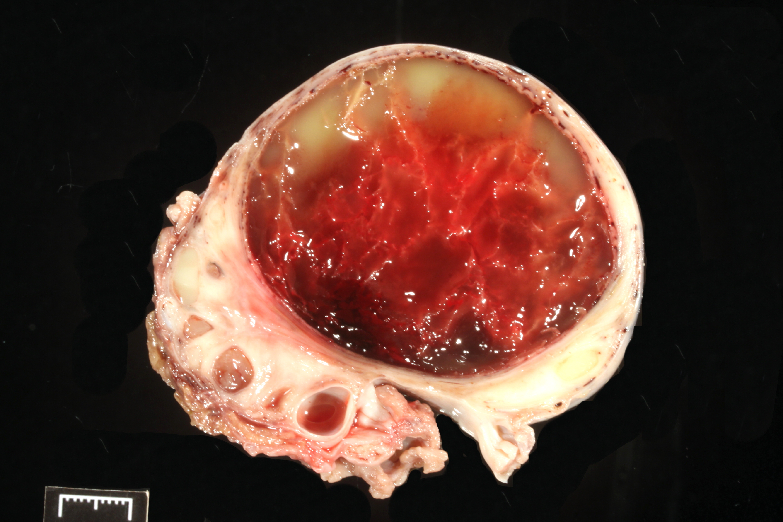
GENITAL: The left ovary (268 g) is oval with a 4.6X4.6X5.2 cm cyst having a 1-2 mm-thick, yellow wall and containing a yellow and red, fibrillary and gelatinous content (submitted).
INTEGUMENTARY/SPECIAL SENSES, MUSCULOSKELETAL, HEMIC & LYMPHATIC URINARY (Right kidney weight: 1.47 kg; Left kidney weight: 1.56 kg), DIGESTIVE, LIVER/PANCREAS (Liver weight: 9.1 kg), NERVOUS (Brain weight: 550 g): No significant findings.
Laboratory results: Hypergammaglobulinemia: globulins 5.4g/dL (92.2-3.8g/dL)
Mature neutrophila PMN 10,153/uL (2260-8580/uL)
Monocytosis 1287/uL (0-1000/uL)
Hyperfibrinogenemia 700mg/dL (100-400 mg/dL)
Thoracocentesis/trans-tracheal wash culture: Streptococcus zooepidemicus 4+, Bacteroides pyogenes 2+ and Fusobacterium spp. 4+
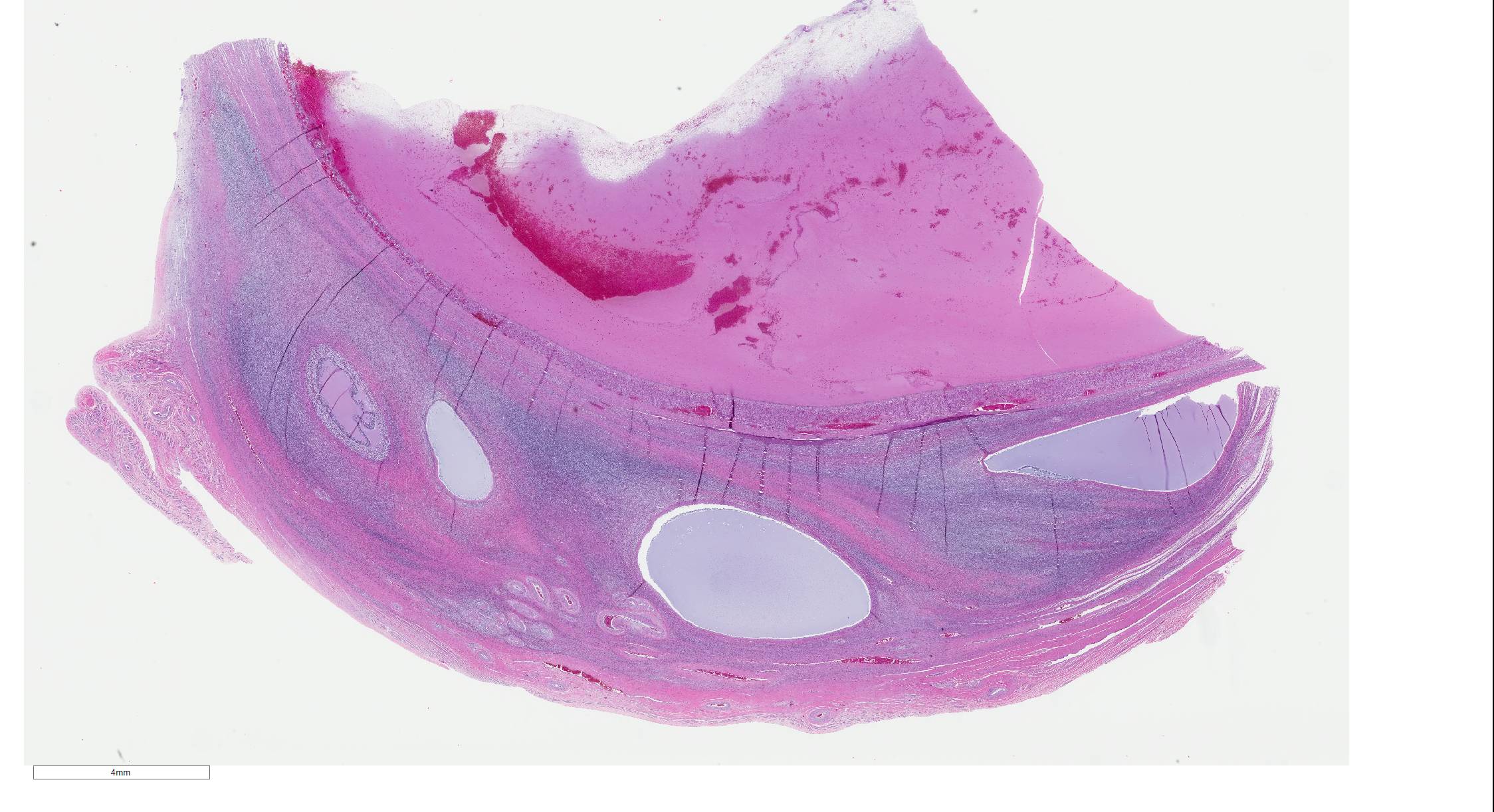
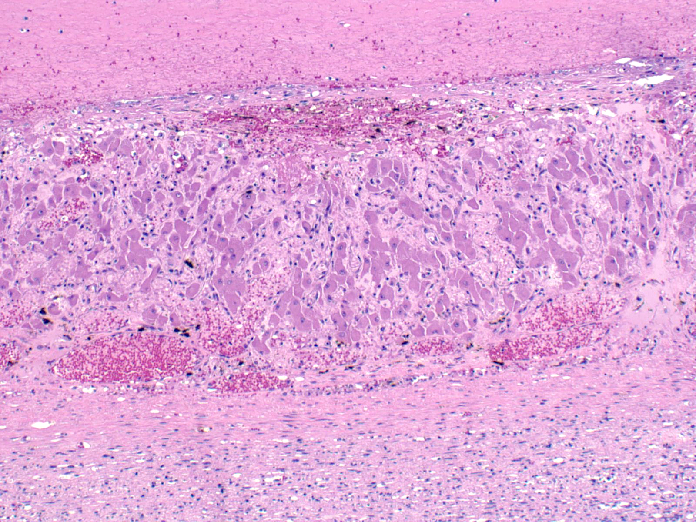
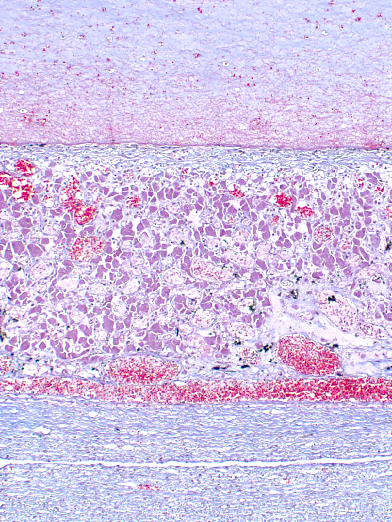
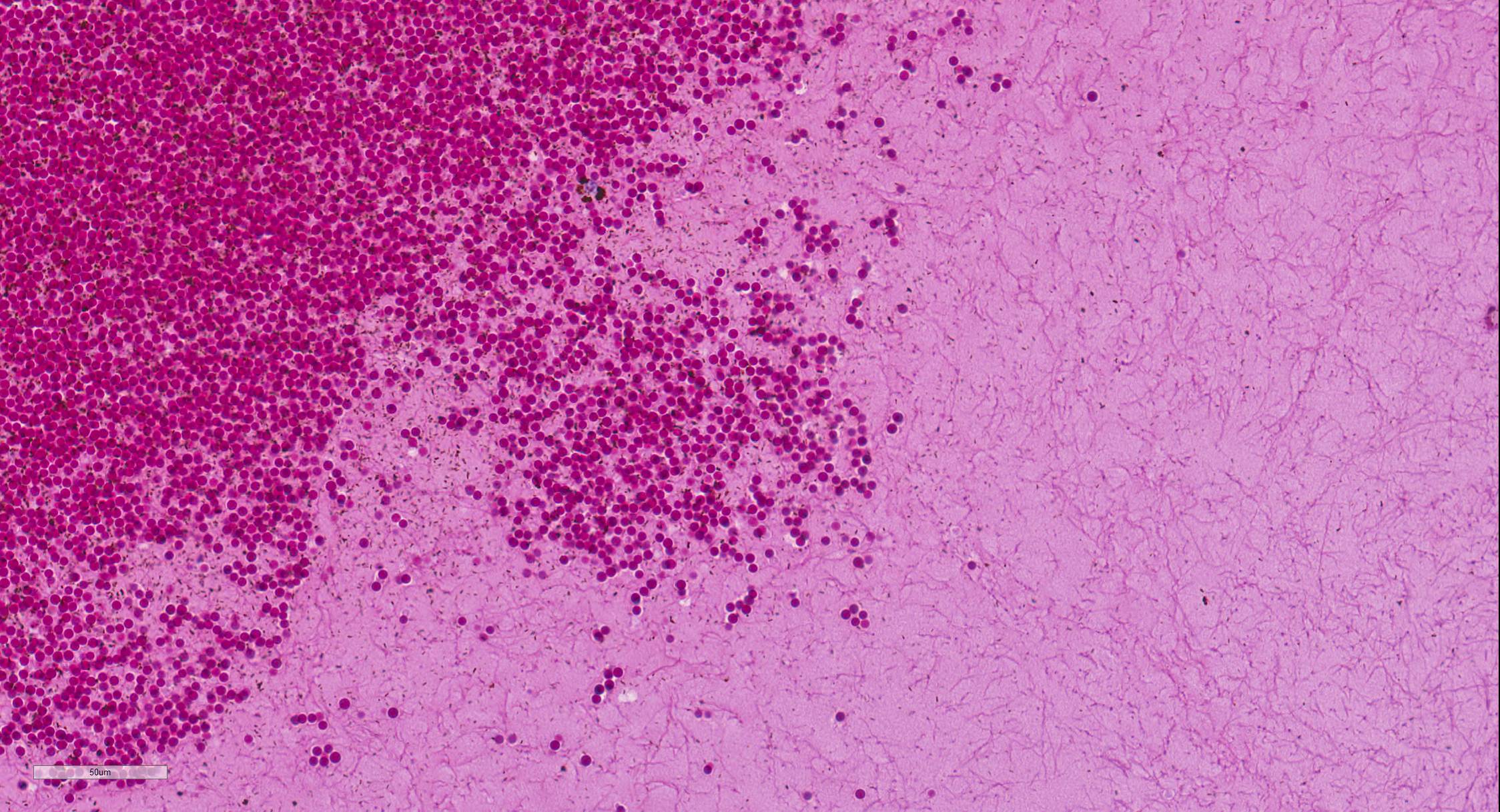
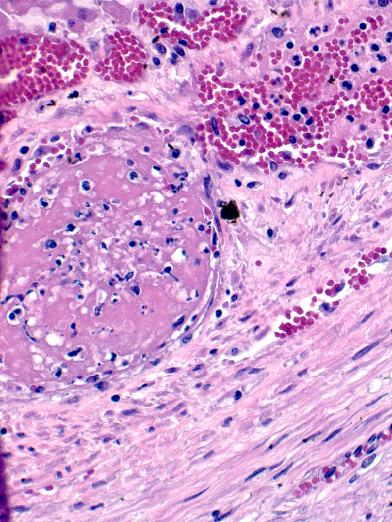
Microscopic Description: Ovary: The section consists of a border of ovarian capsule with a zone of ovarian cortex/stroma containing an occasional egg, various developing and atretic follicles and many hilar vessels. Below this cortical tissue is a band of normal fibromuscular ovarian stroma that ends as a discrete cyst. Moving centripetally into the cyst Is a 5-15 luteal cell-thick lining in a fine, well vascularized stroma and with an inner thin layer of fibrous connective tissue. The central portion of the cyst has pools of free erythrocytes with fine, poorly organized fibrin and fibrillary material. The vessels in the luteal tissue are engorged and several have paucicellular, homogeneous walls (necrosis) with occasionally partial thrombosis. Luteal tissue has some siderophages, but most dark pigment seen is acid hematin. Occasional sections have a hilar artery with segmental, mild, mononuclear cell cuffing.
Contributor Morphologic Diagnosis: Ovarian luteal cyst (Hemorrhagic anovulatory follicle-derived)
Contributor Comment: This is an example of a hemorrhagic anovulatory follicle in the progression of becoming a luteal cyst. Hemorrhagic anovulatory follicles (HAFs) are a common but rarely described lesion seen in equine necropsies and equine biopsy submissions. It is odd that their description is not in veterinary pathology texts.
HAF´s are an "event" described in the current veterinary literature by theriogenologists as a major cause of equine infertility 1,2,3,4,5,6 and most recently in human medicine as a model for women´s luteinized, unruptured-follicle syndrome.1 This "event" must be discussed in view of the horseâs reproductive physiology, because the HAF is similar if not identical to the transitional follicle, an ovarian structure considered normal during the physiologic anovulatory period of the mare during winter´s short photoperiod. Our case occurred at the end of April. The structure should be discussed with an understanding of the equine corpus hemorrhagicum (CH) and corpus luteum (CL). The CH and CL are triangular structures with the apex angled toward the ovulation fossa, and the CH fills in rapidly and usually completely to form a CL 5,7 after ovulation and without significant fibrosis. Theriogenologists know HAFs are a common, if not the most common, lesion associated with anovulation and occur in 5-25% of mares during the breeding season.2.3.4.5.6 In ultrasound of HAFs, the follicular fluid has echogenic foci and swirling fibrin-like strands. Macroscopically on section, the hemorrhagic center is characteristically mottled yellow red, somewhat gelatinous and obviously different from a clot or thrombus. The blood does not flow out of an HAF when it is sectioned. Nor do you see characteristic layering of a large thrombus. Some mares will have several HAFs in a breeding season, and some mares are more predisposed to having them. They are more frequent in old mares. Although, like transitional follicles, HAFs are not treated routinely, some work has been done to discover how to induce them in order the understand the natural pathophysiology of the HAF in the breeding season. Variable success at inducing HAFs has been achieved with administration of prostaglandin, LH and NSAIDs using various regimen. Most recently, dosing mares with the COX-2 inhibitor, flunixin meglumine, resulted in 100% HAF induction.1
When do veterinary pathologists see them? They are common in necropsies of mares with chronic bacterial diseases (like this case) and in cases of endotoxemias and colics. Interestingly, they appear in biopsy services as specimen from ovariectomies where they clinically are diagnosed granulosa cell tumors by rDVM´s. In such biopsy cases, history of an episode of colic in the previous 10 days is common/predictable. One can certainly think that products of sepsis and endotoxemias could both disrupt adenohypophyseal hormone release and generate interleukins and prostaglandins with the result of an anovulation. Most recently, our lab also sees them in ovaries coincident with abscesses induced by follicular aspirations, an increasingly common manipulation.
Are HAFs related to luteal cysts? The luteal tissue is well-vascularized and with DIC, hemorrhage accumulates in follicles that do not ovulate. Had the mare of this case survived, the hemorrhage would have increased due to the vascular lesions you see in the luteal wall. Follicle-sized cysts later form larger, spherical, blood-filled luteinized cysts. It is a rare ovarian hematoma that does not have a luteinized wall.a
The old mantra was that "cystic ovarian disease as described in the cow does not occur in the mare",7 but there may be more similarities than previously believed. This is a case of an HAF progressing into a luteinized cyst and/or ovarian hematoma, but looked at from a pathologist´s perspective and taken from a necropsy case.
Contributing Institution:
Texas A&M University, College of Veterinary Medicine and Biomedical Sciences (Departmental Web site address): http://vetmed.yamu.edu/vtpb
JPC Diagnosis: Ovary: Hemorrhagic luteal cyst (hemorrhagic anovulatory follicle OK)
JPC Comment: The
contributor brings up excellent points on a fairly common cause of ovulation
failure in older mares that rarely merits more than a line in most pathology
texts. This lesion is a rarity in most surgical biopsy practices as especially
as it is often successfully treated with prostaglandin therapy. It is most
often seen as an incidental finding at autopsy, especially in animals dying
suddenly of other causes.
Anovulatory hemorrhagic follicles (AHF), also known as persistent anovulatory
follicles, will grow (especially during transition phases of spring and autumn)
but fail to rupture, and has been estimated to occur between 4.4-13% of all
ovulations in mares, with the higher percentages seen in older mares.4
While the true cause of this lesion is not known, quite a few theories abound
as to its development. These include: a) insufficient gonadotrophic
stimulation to induce ovulation; b) reduced follicular secretion of estrogen;
c) physical blockage of passage of the developing follicle to the ovarian fossa;
d) aberrant production of matrix metalloproteinases, required for tissue
remodeling during ovulation and corpus luteal production, or e) overuse of
ovulation-stimulating drugs, or f) abnormalities in angiogenesis during corpora
lutea formation, or vascular regression during luteolysis.4
This slide is an excellent example of an AHF, with the characteristic wall
consisting of a thin inner fibrovascular layer and a thicker outer layer of
luteinized cells which is heavily vascularized and may be the source of
significant ovarian hemorrhage which may be life-threatening.
Immunohistochemistry is not generally necessary for diagnosis, but these
follicles often express an immunohistochemical profile similar to normal
luteinized cells of corpora hemorrhagica and corpora lutea, with the exception
of a decreased expression of Flk-1, a receptor for vascular endothelial growth
factor (VEGF).4
The moderator commented briefly on the presence of thrombosed capillaries
within this layer of luteinized cells surrounding the HAF, ascribing the
thrombosis to the sepsis seen in this horse rather than the degeneration of the
HAF itself.
References:
1.Bashir ST, Gastal, MO,Tazawa SP, Tarso SGS, Hales DB, Cuervo-Arango J, Baerwald AR, Gastal EL. The mare as a model for luteinized unruptured follicle syndrome: intrafollicular endocrine milieu. Reproduction 2016 151: 271-83.
2.Cuervo-Arango J, Newcombe JR. Risk Factors for the Development of Haemorrhagic Anovulatory Follicles in the Mare. Reprod Dom Anim 2010 45:473â480.
3.Cuervo-Arango J, Newcombe JR. Ultrasound Confirmation of Ovulation in Mares: A Normal Corpus Luteum or a Haemorrhagic Anovulatory Follicle? Reprod Dom Anim 2013 48:105-11.
4.Ellenberger C, Muller K, Schoon H-A, WilsherSR, Allen WR. Histological and Immunohistochemical Characterization of Equine Anovulatory Haemorrhagic Follicles (AHFs). 2008.44:395-405.
5.Ginther OJ, Gastal EM, Gastal MO, Beg MA. Incidence, Endocrinology, Vascularity, and Morphology of Hemorrhagic Anovulatory Follicles in Mares. J EQ Vet Sci 2007 27:130-139.
6.McCue PM, Squires EL. Persistent anovulatory follicles in the mare. Theriogenol 2002. 58:561-43.
7.Roberts SJ. Veterinary Obstetrics and Genital Diseases (Theriogenology). 1986 David and Charles Inc. North Pomfret, VT, pp 585- 587.
a. JF Edwards Platform Presentation: "Transitional ("Autumn") Follicles in the Mare." 39th Annual Meeting Am. College of Veterinary Pathologists, Kansas City, MO, 11-3-1988.