Joint Pathology Center
Veterinary Pathology Services
Wednesday Slide Conference
2017-2018
Conference 13
January 3rd, 2018
CASE I: 14/327 (JPC 4050462).
Signalment: 12 year-old, male, Cairn terrier, Canis familiaris, canine.
History: The dog was examined at the veterinary school at Norwegian University of Life Sciences due to eye problems and was diagnosed clinically with ocular melanosis/melanocytic glaucoma bilaterally but more extensive in the right eye. Eye examination revealed right side buphthalmos +2, right side moderately mydriatic irresponsive pupil, left side iatrogenic miosis, IOP 37/23, diffuse endothelial edema; right side +2-3 and left side +1-2, vitreous prolapse right side and posterior lens luxation, and dorsally ectatic and black pigmented sclera was noted. Black pigmentation also involved conjunctiva. Attempts at controlling the intraocular pressure in the right eye was not successful, and the right eye was enucleated. The owners were informed that lesions also in the left eye most likely would progress.
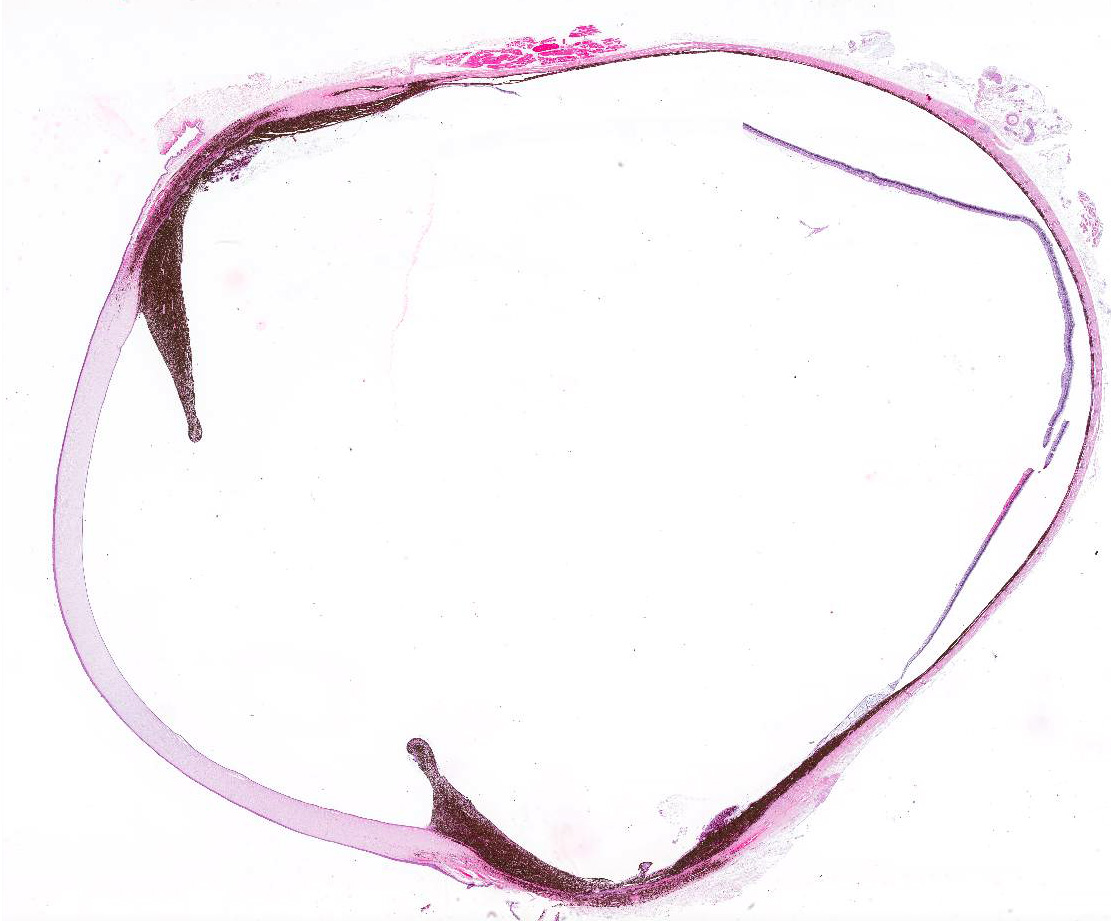
Gross Pathology: An enucleated right eye was received for histopathologic evaluation. The globe measured 2.5 cm in diameter. In the medial canthus of the eyelids, there was a 3mm exophytic tumor with a black surface. The third eyelid was diffusely black without discernible thickening of the tissue. In the globe there were four slightly bulging areas in the anterior portion of the sclera, each 3-4 mm in diameter, with black discoloration of the surface of the sclera, and trans-scleral black discoloration on the cut surface. Anterior vitreous prolapse was not obvious after sectioning of the eye and the lens was detached (thus not included in the sections). A few small opaque areas were detected in the periphery of the lens.
Laboratory results:
None provided.
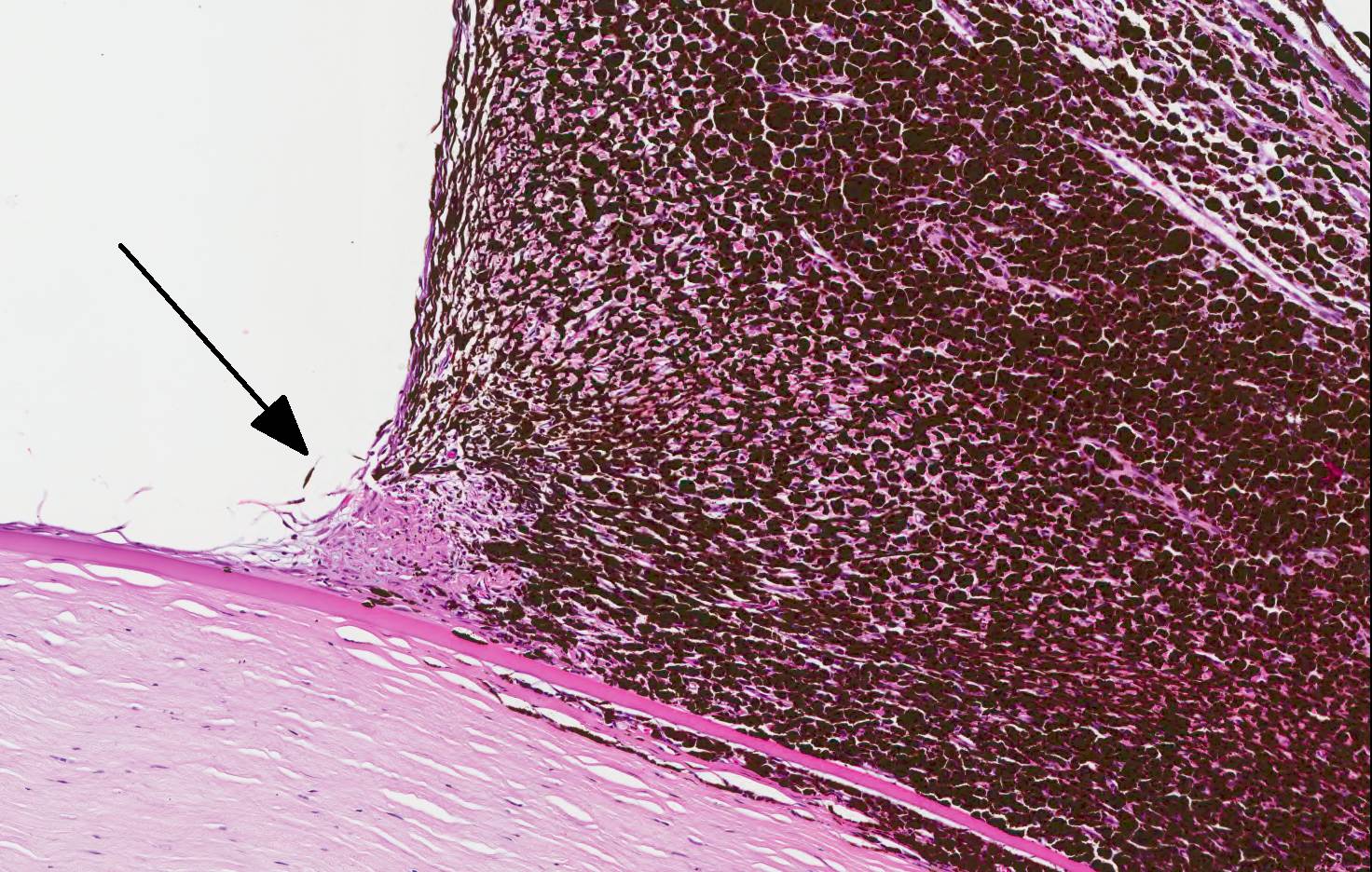
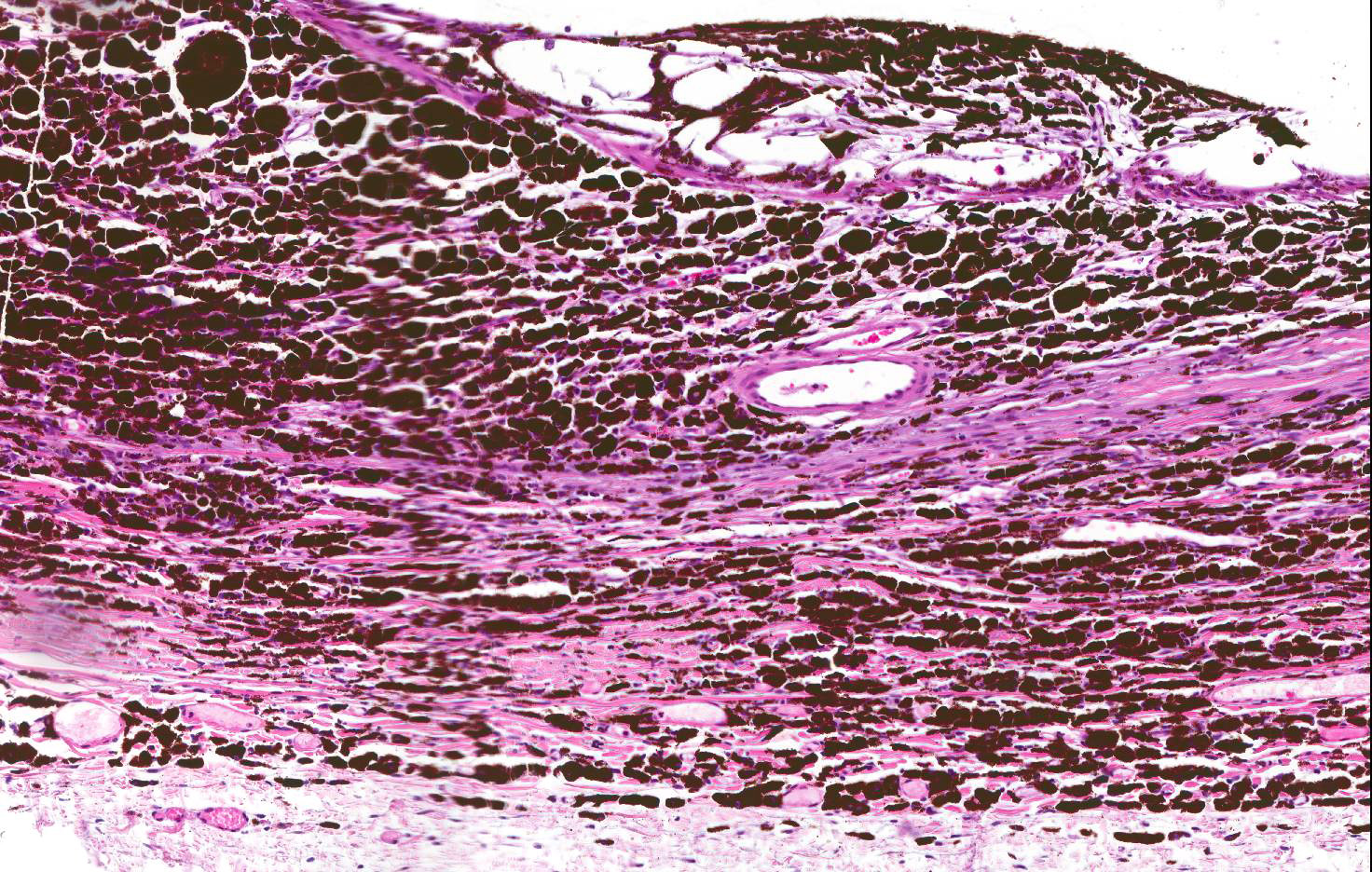
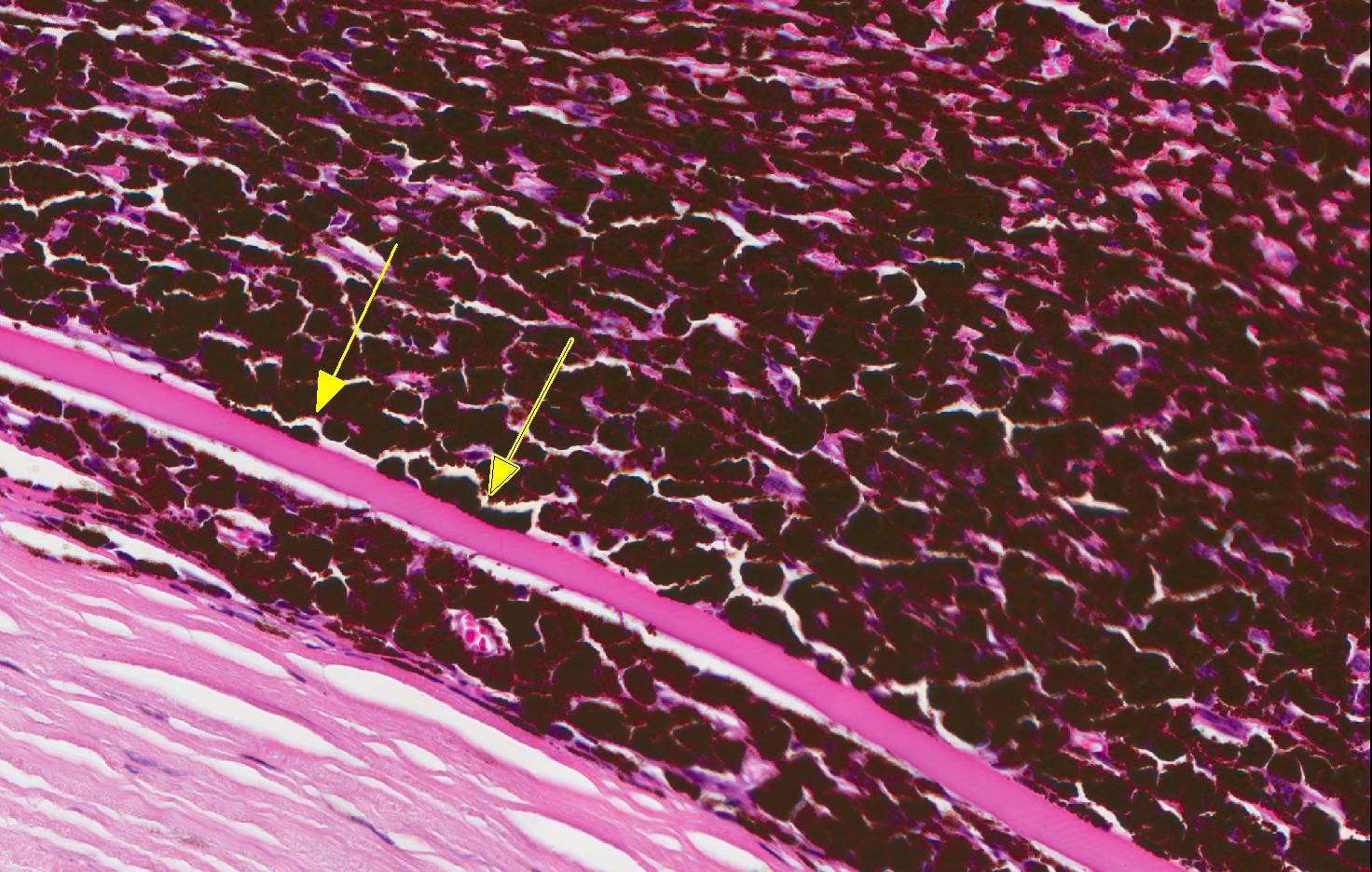
Microscopic Description: In the iris, ciliary body and filtration angle there was a diffuse infiltration of large round plump pigmented cells. Close to the filtration angle, the cells also focally infiltrated the cornea, between Descemet's membrane and corneal stroma. At the anterior portion of the sclera, at the level of iris and ciliary body, there was transscleral infiltration of pigmented cells with separation and loss of scleral connective tissue. Pigmented cells also extended into episclera in some areas. The pigmented cells had abundant cytoplasm with numerous dark brown granules that was bleached by potassium permanganate and a central or peripheral round vesicular nucleus with a small nucleolus. The mitotic index was <1 per 10 HPFs, and minimal anisocytosis and anisokaryosis. The retina was detached (artifact). There was degeneration and loss of neurons in the ganglion layer, moderate thinning of the inner granular layer and mild multifocal fusion of inner and outer nuclear layer in the retina. In the anterior and posterior chambers a pale blue material (vitreous) with some free pigmented cells.
In the lens (not submitted) there was multifocal degeneration of stroma on the anterior side and swollen lens fibers (Morgagnian globules) and large eosinophilic swollen cells (bladder cells).
On the rim of the eyelid from medial canthus there was a focal hyperplasia of sebaceous glands with lobules of well differentiated glandular tissue surrounding a centrally located duct (not submitted). In the surrounding dermis in this area and diffusely in the medial conjunctiva, including the third eyelid, there was multifocal to confluent infiltration of pigmented cells as described above.
The globe was re-embedded in a standard size tissue block, and this caused an artificial dorsoventral flattening of the globe.
Contributor’s Morphologic Diagnosis:
Eye: Ocular melanosis with secondary glaucoma.
Contributor’s Comment: The lesions in this specimen are consistent with the condition called ocular melanosis of Cairn terriers. In a study describing the clinical presentation of 114 Cairn terriers diagnosed with ocular melanosis, the earliest lesions was dark-colored thickening of the iris root followed by scleral/episcleral pigment plaques, release of pigment into the aqueous and deposition in the drainage apparatus, especially ventrally.3 In advanced cases, secondary glaucoma develops, and 3 of the 114 dogs developed uveal melanocytic neoplasms.3
Ocular melanosis is characterized by diffuse infiltration of plump pigment-laden cells mainly in anterior segments of the eye including the iris, ciliary body, sclera/episclera overlying the filtration angle and the peripheral deep layers of the cornea, but posterior segments may also be involved.4
An important differential diagnosis is uveal or limbal melanocytoma in the dog, as the pigmented cells infiltrating ocular tissue in ocular melanosis are histologically similar to such tumor cells. However the growth pattern is reported to be different; in ocular melanosis the pigmented cells infiltrate diffusely in the tissues, as opposed to uveal or limbal melanocytomas in which the tumor cells are expected to result in an expanding mass.4
The origins of the pigment-laden cells have been controversial, and the main cell population has been described to be dominated by either melanophages or melanocytes. Van de Sandt et al6 described the ultrastructural morphology of most of the cells to be consistent with melanophages and some cells appearing to be melanocytes. In this paper, the specific origin of ocular tissue chosen for electron microscopy study was not indicated. In another study4 where iridal and ciliary body tissue was ultrastructurally investigated, the main cell population was described as melanocytes containing melanosomes in stage III or IV of development, but some cells that probably represented melanophages were also observed. Both Van de Sandt et al6 and Petersen-Jones et al4 reported the cells to be negative for the common melanocyte marker Melan A. However, Petersen-Jones et al4 described most but not all cells to be immunohistochemically positive for HMB45, an antibody that recognizes gp100, which is a melanosome organelle specific marker localized in stage II and III melanosomes. Some cells were also positive for MITF, a melanocytic nuclear transcription factor. Most eyes contained some pigmented cells positive for CD18 suggestion they were macrophages that had engulfed pigment, but in 1 globe which was markedly inflamed, out of 8 globes investigated immunohistochemically, there were abundant CD18 positive pigmented cells.4
The cause of the disease is unknown. The disease is reported to be inherited with a possible autosomal dominant mode of inheritance.3 In one study examining 11 potential candidate genes, none of the selected candidate genes were likely to be the gene locus for ocular melanosis in Cairn terriers.7
JPC Diagnosis: Globe, anterior uvea, choroid, and sclera: Melanosis with anterior synechae formation and drainage angle occlusion with mild to moderate diffuse retinal atrophy, Cairn terrier, canine.
Conference Comment: Ocular melanosis, also known as pigmentary glaucoma, most commonly occurs in the Cairn terrier breed and results in excessive pigmentation of the uvea which disrupts the contour of the uvea particularly prominent at the iris base, anterior ciliary body and limbal sclera. The pigmented cells have been identified through electron microscopy and immunohistochemistry to be melanocytes or melanophages (described in more detail above). The thickened limbal scleral and episclera can give the impression of neoplasia; however, melanocytoma (the most likely differential) can be distinguished from melanosis by the presence a regional mass that compresses adjacent tissues. In contrast, melanosis is more diffuse and often bilateral in the Cairn terrier. Ocular melanosis has also been identified in other breeds such as the Boxer and Labrador Retriever, and in these breeds is clinically and morphologically similar, varying only in the distribution. In other breeds, melanosis is usually unilateral and composed predominately of melanophages based on limited electron microscopic studies.2
The eyelid and brow may also be involved, in which the condition is known as oculodermal melanocytosis, which correlates with a high risk for melanoma in Caucasian patients.2 In dogs, there have been occasional reports of melanocytoma or malignant uveal melanoma occurring in eyes simultaneously affected with melanosis. A recent article1 reports a Golden Retriever with diffuse ocular melanosis and extension into the bulbar conjunctiva and orbital space forming a pigmented, necrotic mass diagnosed as a limbal melanocytoma. Remarkably, there was also a pigmented mass in the third eyelid of the opposite eye that was also diagnosed as a melanocytoma. Cases such as this give weight to the belief of some pathologists that ocular melanosis is merely diffuse melanocytoma.2
Ocular melanosis results in a slowly progressive chronic glaucoma associated with compression of and accumulation of pigmented cells within the filtration angle and scleral venous plexus. Free melanin granules are often present and are phagocytized by local macrophages and trabecular endothelial cells within outflow tracts. Secondary glaucoma of this nature is not responsive to medical or surgical treatment because melanophages and melanocytes continue to proliferate and eventually abrogate the treatment by obstructing whatever therapeutic intervention was initiated.5 In humans, ocular melanosis occurs rarely and results in unilateral heterochromia of the iris and a darkened choroid.
Canine glaucomas are classified based on the following criteria: possible cause (primary, secondary, or congenital), gonioscopic appearance of the filtration angle, and duration or stage of disease. Primary glaucomas are characterized by intra-ocular pressure (IOP) increases without any concurrent disease; these are often hereditary in certain breeds (reported in over 45 breeds, of which the most notable are Beagle, Basset Hound, Welsh springer spaniel and Great Dane) and can occur bilaterally. Primary glaucomas often occur due to pectinate ligament dysplasia or consolidation of ligaments into sheets (mesodermal dysgenesis) or abnormal metabolism of the trabecular cells of the outflow system or pupillary blockage. Secondary glaucomas result from increased IOP associated with concurrent ocular disease, such as uveitis, lens luxations, intumescent cataracts, phacolytic or clastic uveitis, hyphema, intraocular neoplasia or melanosis, which obstruct aqueous outflow pathways. Several breeds are predisposed to lens luxation, most commonly Fox Terrier, Sealyham Terrier, Border Collie, Tibetan Terrier, Cairn Terrier, Welsh Corgi, and Jack Russell Terrier. In Jack Russell Terriers, Miniature Bulldogs, and Lancashire Heelers, a mutation of the ADAMTS17 gene has been associated with lens luxation. Finally, in congenital glaucoma increased IOP is caused by multiple anterior segment anomalies resulting in decreased aqueous humor outflow and develops soon after birth. Congenital glaucoma is exceedingly rare in dogs, whereas, primary (breed-related) and secondary glaucomas are most common.5
Conference participants described peripheral anterior synechiae (Descemet’s membrane extends into the ciliary body), ectropion uveae due to a thin pre-iridal fibrovascular membrane, and evidence of secondary glaucoma (thin sclera and retina). The moderator discussed a proposed grading scheme that has not been published yet for ocular melanosis: increased melanin-containing cells (grade I), increased melanin-containing cells and distortion (grade II), and melanin-containing cells increased and invading sclera (grade III).
Contributing Institution:
References:
- Dees DD, Maclaren NE, Teixeira L, Dubielzig RR. An unusual case of ocular melanosis and limbal melanocytoma with benign intraorbital extension in a dog. Vet Ophthalmol. 2013;16(suppl 1):117-122.
- Dubielzig RR, Ketring KL, McLellan GJ, Albert DM. The uvea. In: Veterinary Ocular Pathology a Comparative Review. New York, NY: Saunders Elsevier; 2010:280-282.
- Petersen-Jones SM, Forcier J, Mentzer AL. Ocular melanosis in the Cairn terrier: clinical description and investigation of mode in inheritance. Vet Ophthalmol. 2007;10(suppl.1):63-69.
- Petersen-Jones SM, Mentzer AL, Dubielzig RR, Render JA, Steficek BA, Kiupel M. Ocular melanosis in the Carin terrier: histopathological description of the condition, and immunohistochemical and ultrastructural characterization of the characteristic pigment-laden cells. Vet Ophthalmol. 2008;11(4):260-268.
- Plummer CE, Regnier A, Gelatt KN. The canine glaucomas. In: Gelatt KN, Gilger BC, Kern TJ, eds. Veterinary Ophthalmology. 5th Vol. 2. Ames, IA: John Wiley & Sons, Inc.; 2013: 1053-1054, 1075-1077, 1100-1101.
- van de Sandt RR, Boevé MH, Stades FC, Kik MJ. Abnormal ocular pigment deposition and glaucoma in the dog. Vet Ophthalmol. 2003;6(4):273-278.
- Winkler PA, Bartoe JT, Quinones CR, Venta PJ, Petersen-Jones SM. Exclusion of eleven candidate genes for ocular melanosis in Cairn terriers. J Negat Results Biomed. 2013;12(6).