Joint Pathology Center
Veterinary Pathology Services
Wednesday Slide Conference
2017-2018
Conference 8
October 25th, 2017
CASE III: P1270-11 (JPC 4018605).
Signalment: 10-year-old, male, neutered, domestic, Felis catus, feline.
History: This cat appeared to be in good health at 1 :00pm; the owner reported he had appeared to sleep more than usual for the last few days. At 1:00am that night, the owner found his cat in severe respiratory distress with sialorrhea. The cat died after an hour with no change in his condition, on its way to the veterinarian.
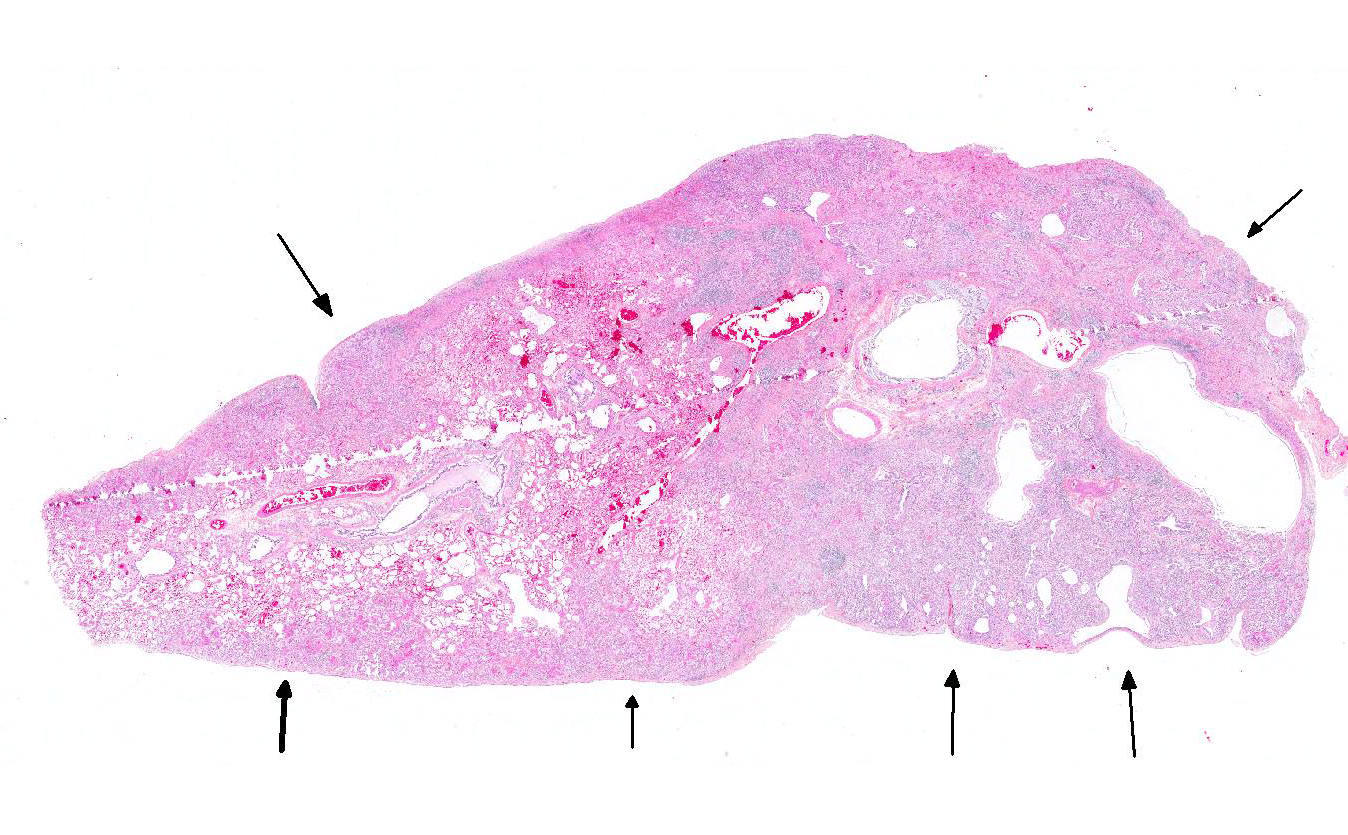
Gross Pathology: The cat was in good body condition. There were numerous firm whitish nodules, 0.5 to 2 mm in diameter, distributed extensively throughout both lungs, with multifocal atelectasis. A mild amount of mucoid material filled the distal trachea.
Laboratory results: Routine bacteriology on the lungs was not significant (rare contaminants), and negative on liver and kidney.
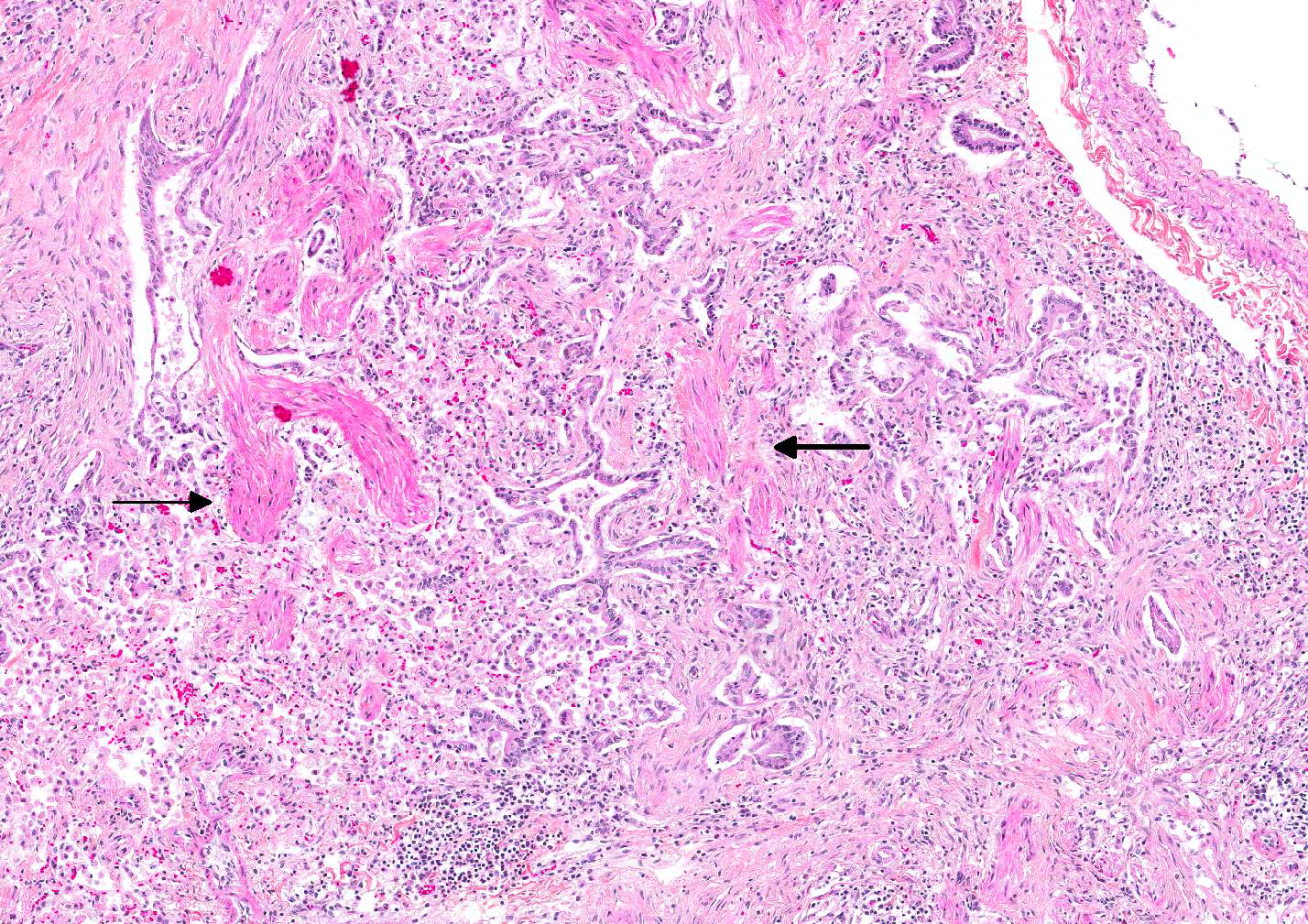
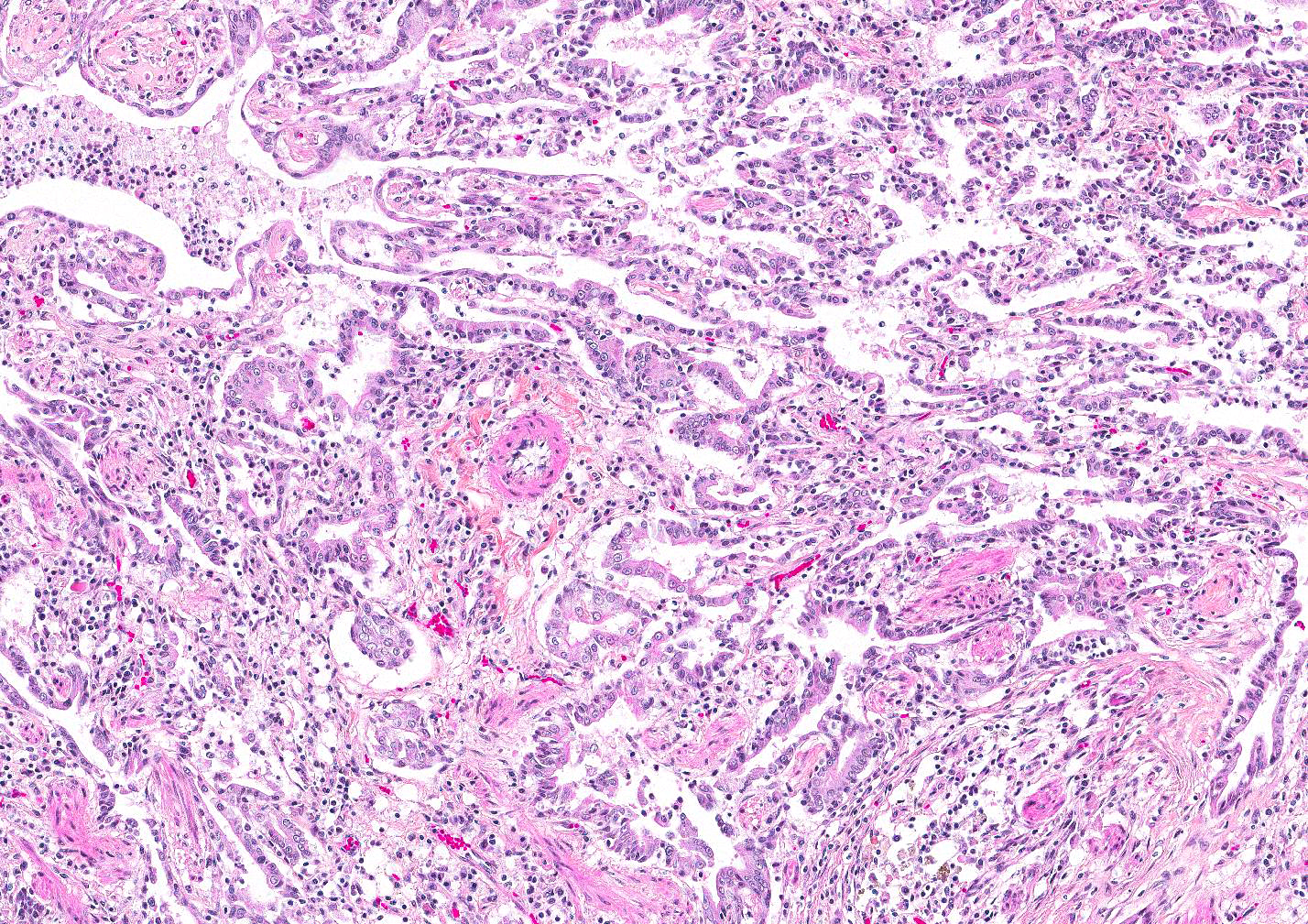
Microscopic Description: Lung: There is extensive multifocal remodeling of the pulmonary parenchyma, more severe in subpleural areas. The alveolar septa and distal airways are distorted and moderately expanded by dense collagen (fibrosis), smooth muscle bundles and, variably, clusters of mesenchymal cells (fibroblasts/myofibroblasts); they are lined by cuboidal to columnar epithelial cells, and multifocally form larger tubular structures (honeycomb pattern). The alveoli and bronchioles in affected areas are occasionally filled with plump macrophages, and rare to few neutrophils. The epithelium of several, usually larger bronchioles have several goblet cells (mucous metaplasia) and a few foci of squamous metaplasia are visible. There are multifocal moderate lymphoplasmacytic interstitial and subpleural infiltrates. The pleura is multifocally covered by cuboidal to low columnar (hypertrophied) mesothelial cells. There is some variation between the 2 sections/slides submitted. In one of the sections, there is a focal bronchiolo-alveolar proliferation with minimal stroma, suggesting bronchiolo-alveolar adenoma or carcinoma, and focal mucopurulent bronchitis. In the other section, there is multifocal mineralization.
Contributors Morphologic Diagnosis: Lung: Extensive, multifocal, moderate to marked interstitial pulmonary fibrosis with smooth muscle hyperplasia/metaplasia, epithelial hyperplasia/metaplasia, and fibroblast/myofibroblast foci (probable bronchiolo-alveolar adenoma or carcinoma in one section).
Contributors Comment: The histological changes in this lung are consistent with feline idiopathic pulmonary fibrosis (FIPF), a previously reported feline interstitial lung disease. Interstitial lung diseases (ILDs) are a heterogeneous group of disorders affecting the pulmonary interstitium, more precisely the alveolar wall, with a variety of etiologies; however, the cause often remains unknown. Most ILDs result from exaggerated inflammatory and reparative responses to an initial insult, which may be infectious, toxic or environmental2. Immune-mediated connective tissue disorders result in ILDs in humans and perhaps in dogs; a similar role in feline pulmonary disease has been suggested but has not been proven2. In veterinary medicine, lung diseases with a prominent fibrotic component of unknown etiology are often called idiopathic pulmonary fibrosis (IPF). In humans, at least four distinct entities used to be classified as IPF, including usual interstitial pneumonia (UIP)4. A consensus statement established by the American Thoracic Society and the European Respiratory Society defined the criteria for the diagnosis of IPF in humans and eliminated all but UIP from the definition of IPF. The histologic features of UIP lungs are temporal heterogeneity of lung remodeling, with the primary changes being interstitial fibrosis and ongoing fibroblast/myofibroblast proliferation, metaplasia of the alveolar epithelium (honeycomb change with enlarged airspaces lined by prominent variable epithelium), and scant inflammation4.
Feline idiopathic pulmonary fibrosis (FIPF) is an uncommon chronic interstitial lung disease associated with chronic progressive tachypnea, respiratory distress and cough in middle-aged to older cats2. Contrary to other ILDs, IPF is believed to be a fibroproliferative disorder. FIPF type II pneumocyte ultrastructure revealed abnormal dense cytoplasmic lamellar body-like inclusions; this finding is similar to a heritable form of human IPF and is possibly related to a defect in type II pneumocyte biology4. FIPF is defined by histopathologic characteristics of usual interstitial pneumonia (UIP). Lesions can be diffuse or patchy. Type II pneumocyte and myofibroblasts are important cellular constituents of feline IPF. Williams reported that myofibroblasts were prominent in foci, beneath honeycombing and hyperplastic epithelium, and in alveolar septa away from the remodeling4. An association between pulmonary fibrosis and carcinoma is recognized in humans and animals. Cohn described an IPF-like condition with a coincident pulmonary neoplasia in 6 of 23 cats2. These pulmonary neoplasms were generally located in areas of marked fibrosis but the neoplastic foci were limited in extent. Hypotheses to explain coexistence of lung cancer and fibrotic ILD include progression of epithelial hyperplasia to neoplasia, shared etiologic risk factors, and induction of carcinogenesis by diffuse inflammation.
Another idiopathic ILD, diagnosed as the desquamative form of cryptogenic fibrosing alveolitis has been described in a single cat3. Idiopathic fibrotic ILD has been described in the dog (West Highland White Terrier). It is characterized by progressive and poorly responsive interstitial fibrosis1. However, the condition in dogs is not histologically equivalent to UIP since it lacks alveolar metaplasia, smooth muscle hyperplasia or metaplasia and foci of ongoing fibrosis2. Equine multinodular pulmonary fibrosis is another progressive fibrotic lung diseases that has been associated with an EHV-5 virus1.
JPC Diagnosis: Lung: Fibrosis, interstitial, subpleural, multinodular, severe with marked alveolar loss, bronchiolarization and bronchiolar epithelial metaplasia, and arteriolar and bronchiolar smooth muscle hyperplasia, domestic (Felis catus), feline.
Conference Comment: In contrast with case I (equine multinodular pulmonary fibrosis), this disease entity results in progressive fibrosis with areas of less mature fibrous connective tissue adjacent to mature collagen. The moderator commented that there is very little inflammation in these cases which rules out the possibility of post-inflammatory remodeling. There is also occasional traction bronchiectasis present which is caused by contraction of the fibrous connective tissue pulling apart bronchioles.
There were no pulmonary adenomas or adenocarcinomas in our sections, although it is entirely possible that it was present in the sections viewed by the contributor. Commonly, epithelial hyperplasia associated with this entity is mistaken for a neoplasm; however, IPF can predispose cats to pulmonary adenocarcinoma due to chronic fibrosis and remodeling of the airways.1
University of Montreal
College of Veterinary Medicine
References:
1. Caswell JL, Williams KJ. Respiratory system. In : Maxie MG, ed. Jubb, Kennedy, and Palmers Pathology of Domestic Animals. 5th ed. Vol. 2. Philadelphia, PA: Saunders Elsevier; 2007; 496, 523-653.
2. Cohn LA, Norris CR, Hawkins EC, et al. Identification and characterization of an idiopathic pulmonary fibrosis-like condition in cats. J Vet Intern Med. 2004;18:632641.
3. Rhind SM, Gunn-Moore DA. Desquamative form of cryptogenic fibrosing alveolitis in a cat. J Comp Pathol. 2000;123:226229.
4. Williams K, Malarkey D, Cohn L, et al. Identification of spontaneous feline idiopathic pulmonary fibrosis morphology and ultrastructural evidence for a type II pneumocyte defect. Chest. 2004;125:22782288.