Signalment:
Four-year-old, spayed female domestic medium hair cat (
Felis cats), feline.The history described facial dermatitis that progressed over a four-month period to generalized erythema and crusting of the pinnae, paws, dorsum, legs, and ventrum. Euthanasia was elected due to progressive deterioration of the cat.
Gross Description:
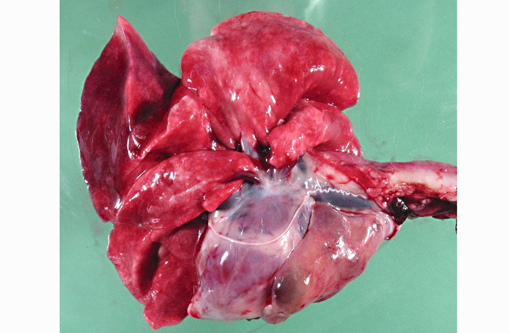
The body was in good postmortem condition. Thick sheets of exfoliated keratin or tan to yellow exudate covered regions of alopecia and erythema on the legs, ventral and lateral abdomen and thorax, dorsum, muzzle, and pinnae. The residual hair coat was easily epilated and often entrapped thick layers of keratin. The cranial mediastinum contained a 5.5 x 3 x 2 cm, pale red to tan mass. The mass contained multiple cystic structures that were separated by soft pale red parenchyma and filled with translucent pale yellow to blood-tinged fluid.
Histopathologic Description:
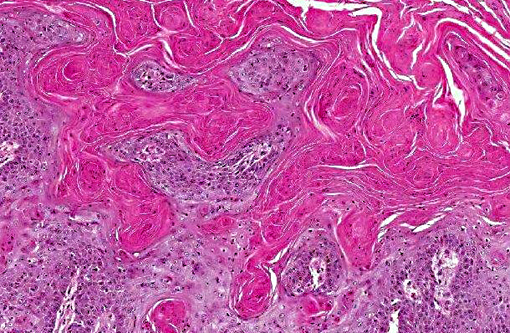
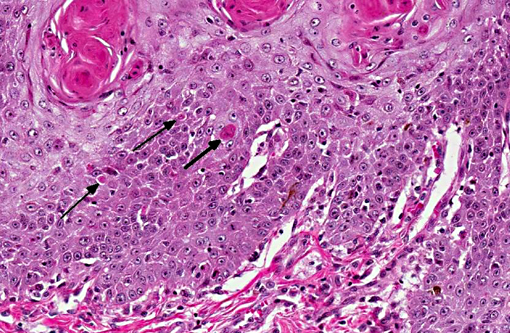
There was severe, diffuse, compact, orthokeratotic to parakeratotic hyperkeratosis that covered the epidermis and extended into most follicular infundibula which often lacked hair shafts. The epidermis was moderately to markedly acanthotic with prominent rete pegs. The epidermis was segmentally eroded to ulcerated and covered by thick serocellular crusts admixed with colonies of gram positive cocci. There were scattered individual necrotic keratinocytes in the stratum spinosum, and less frequently in the stratum basale and stratum granulosum. Lymphocytes were multifocally exocytosed into the stratum basale and the deep layers of the stratum spinosum. The dermis was moderately inflamed with a perivascular distribution of mast cells, plasma cells, and fewer lymphocytes. Sebaceous glands were diffusely atrophied.Â
Morphologic Diagnosis:
Skin: Epidermal hyperkeratosis and acanthosis with apoptotic keratinocytes, lymphoplasmacytic perivascular dermatitis, and sebaceous gland atrophy.
Condition:
Thymoma and exfoliative dermatitis
Contributor Comment:
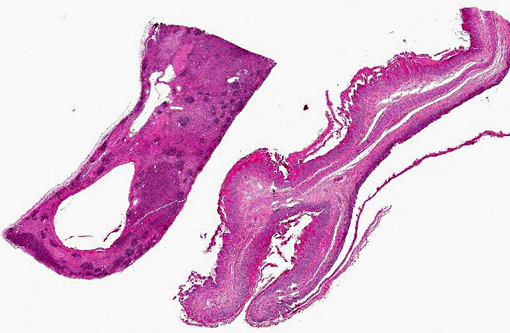
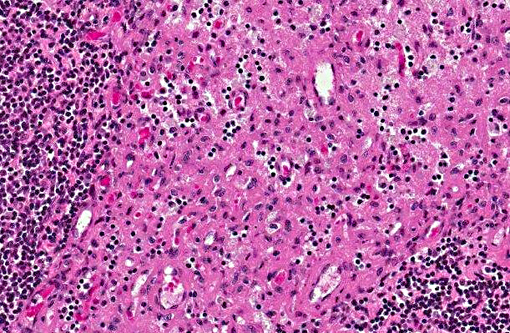
The mediastinal mass was composed of dense aggregates of small to medium-sized lymphocytes that were surrounded by sheets of larger polygonal to round cells with moderate to abundant pale eosinophilic cytoplasm, ovoid to indented hypochromic nuclei, and 0-1 basophilic nucleoli. These larger polygonal cells demonstrated cytoplasmic immunoreactivity for pancytokeratin, facilitating the diagnosis of a thymoma. Thymomas arise from thymic epithelial cells and are classified as lymphocytic, epithelial, or mixed based on the ratio of epithelial cells to lymphocytes.(4) Thymomas are exceedingly rare in cats and are seen most often in middle-aged to older animals. Several immune mediated conditions in humans, dogs, and cats have been associated with thymomas, including myasthenia gravis, polymyositis, and various dermatoses.(6)
Thymoma-associated exfoliative dermatitis is an uncommon condition that has been reported in cats and rabbits.(1,5,6) This disorder is thought to be a paraneoplastic syndrome that results from the failure of the neoplastic thymus to eliminate autoreactive T lymphocytes that target epidermal keratinocytes.(3,5) The association between exfoliative dermatitis and thymomas has been supported clinically by the alleviation of cutaneous lesions following surgical removal of the thymoma.(5)
The cutaneous lesions of erythema and exfoliation of keratin are often first noted on the head, neck, and pinnae, but progressively become more generalized.(3) Alopecia is commonly seen as a sequela to the exfoliative dermatitis.(3) Clinical differentiation from other exfoliative dermatoses can be achieved by skin biopsies and a diagnosis of thymoma via thoracic radiographs and fine needle aspirates of the mass.(3)
The typical histopathologic lesions of thymoma-associated exfoliative dermatitis include severe parakeratotic to orthokeratotic hyperkeratosis, acanthosis, mild transepidermal apoptosis, sebaceous gland atrophy, and cell-poor interface dermatitis.(3,5) An alternative diagnosis to consider is the hyperkeratotic form of erythema multiform.(3) Both conditions can exhibit marked hyperkeratosis and variable degrees of interface dermatitis, but transepidermal apoptosis is often more severe in erythema multiform.(3)
JPC Diagnosis:
1. Thymus: Thymoma.
2. Haired skin, auricular pinna: Epidermal hyperplasia and hyperkeratosis, diffuse, marked, with multifocal keratinocyte necrosis and mild cell-poor lymphoplasmacytic interface dermatitis.Â
Conference Comment:
In an informative summary of this rare condition, the contributor notes that thymoma-associated exfoliative dermatitis is typically characterized by parakeratosis and a cell-poor interface dermatitis; however, in a review of five cats with this paraneoplastic condition, Rottenberg et al also observed examples of cell-rich skin lesions.(5) Conference participants discussed the use of the terms cell-poor and cell-rich in defining and categorizing various types of interface dermatitis. Interface dermatitis refers to conditions in which an inflammatory infiltrate abuts and/or obscures the dermoepidermal junction; it is classified based on the dominant inflammatory cell type involved (i.e. neutrophilic, lymphocytic, lymphohistiocytic, etc.), and can be further described as either cell-poor or cell-rich. Cell-poor interface dermatitis is characterized by a sparse infiltrate of inflammatory cells along the dermoepidermal junction, whereas its cell-rich counterpart also referred to as lichenoid interface dermatitis -- comprises a heavy band-like inflammatory infiltrate which can obscure the epidermal basal layers. In humans, cell-poor interface dermatitis is associated with conditions such as erythema multiforme, systemic lupus erythematous, dermatomyositis, mixed connective tissue disease, graft-versus-host disease, morbilliform viral exanthema, and morbilliform drug reactions. Cell-rich interface dermatitis is observed in cases of idiopathic lichenoid disorders, discoid lupus erythematous, lichenoid and granulomatous dermatitis, lichenoid purpura, and lichenoid and fixed drug reactions.(2)
References:
1. Florizoone K. Thymoma-associated Exfoliative Dermatitis in a Rabbit.Â
Veterinary Dermatology. 2005;16:281-284.
2. Crowson AN, Magro CM, Mihm Jr MC. Interface Dermatitis.Â
Archives of Pathology & Laboratory Medicine. 2008;132(4):652-666.Â
3. Gross TL. Ihrke PJ. Walder EJ, et al.Â
Skin Diseases of the Dog and Cat. 2nd ed. Ames, IA: Blackwell Science Ltd; 2005:68-70, 78-79.
4. Jacobs RM. Messick JB. Valli VE. Tumors of the hemolymphatic system. In: Meuten DJ, ed.Â
Tumors in Domestic Animals. 4th ed. Ames, IA: Blackwell Publishing Professional; 2002:165-166.
5. Rottenberg S, Tscharner CV, Rossje RJ. Thymoma-associated Exfoliative Dermatitis in Cats.Â
Vet Pathol. 2004;41:429-433.
6. Scott DW, Yager JA, Johnston KM. Exfoliative Dermatitis in Association with Thymoma in Three Cats.Â
Feline Pract.1995;23:8-13.