CASE 4: OSU 2013 2 (4041565-00)
Signalment: 1-day-old, male, Miniature horse (Equus ferus caballus)
History: A dead, premature Miniature horse colt was delivered on 2/14/13 by a mare that presented with dystocia. The placenta passed approximately 10 minutes post-partum and while it appeared grossly normal, it weighed 6.2 pounds (increased). The mare's due date was 3/8/13. The colt and placenta presented for a complete necropsy on 2/15/13.
Gross Pathology: The body condition score was 1.5/5 and the animal presented in good post-mortem condition. A mild amount of yellow-brown, soft material was present on the tail, perineum, and all four limbs.
The endocardium of the heart contained two areas of red discoloration that extended 1-2 mm within the myocardium. The first area measured 5 x 5 mm and was located just ventral to the mitral valve; the other are measured 5 x 8 mm and was present within the papillary muscle. Bilaterally, both adrenal glands were characterized by markedly thin cortices, with a cortical to medullary ratio of 1:8. The cortical surface contained hundreds of pinpoint, red foci.
Both tips of the uterine horns contained dozens of raised, firm, tan irregular tissue that was moderately well-demarcated. The amniotic sac contained hundreds of raised, white, pinpoint, soft foci (amniotic plaques).
Microscopic description:
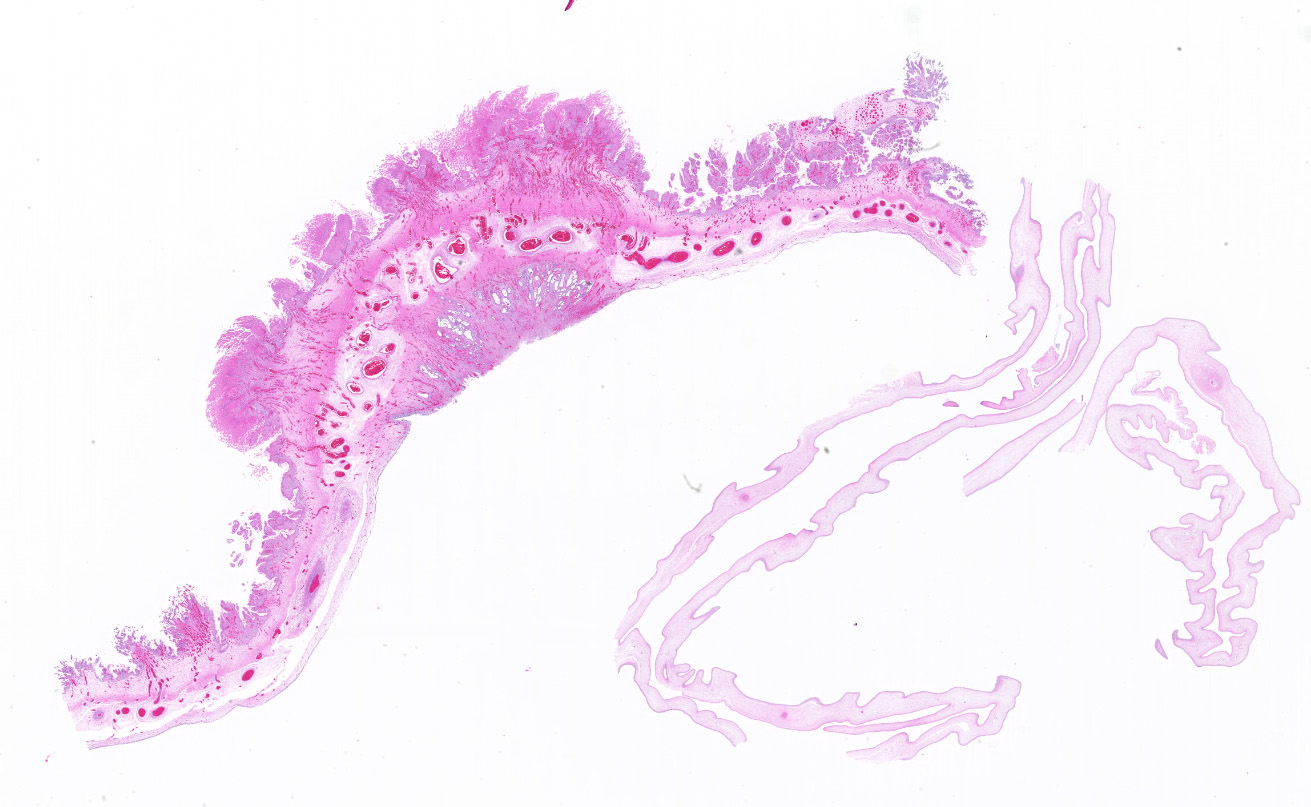
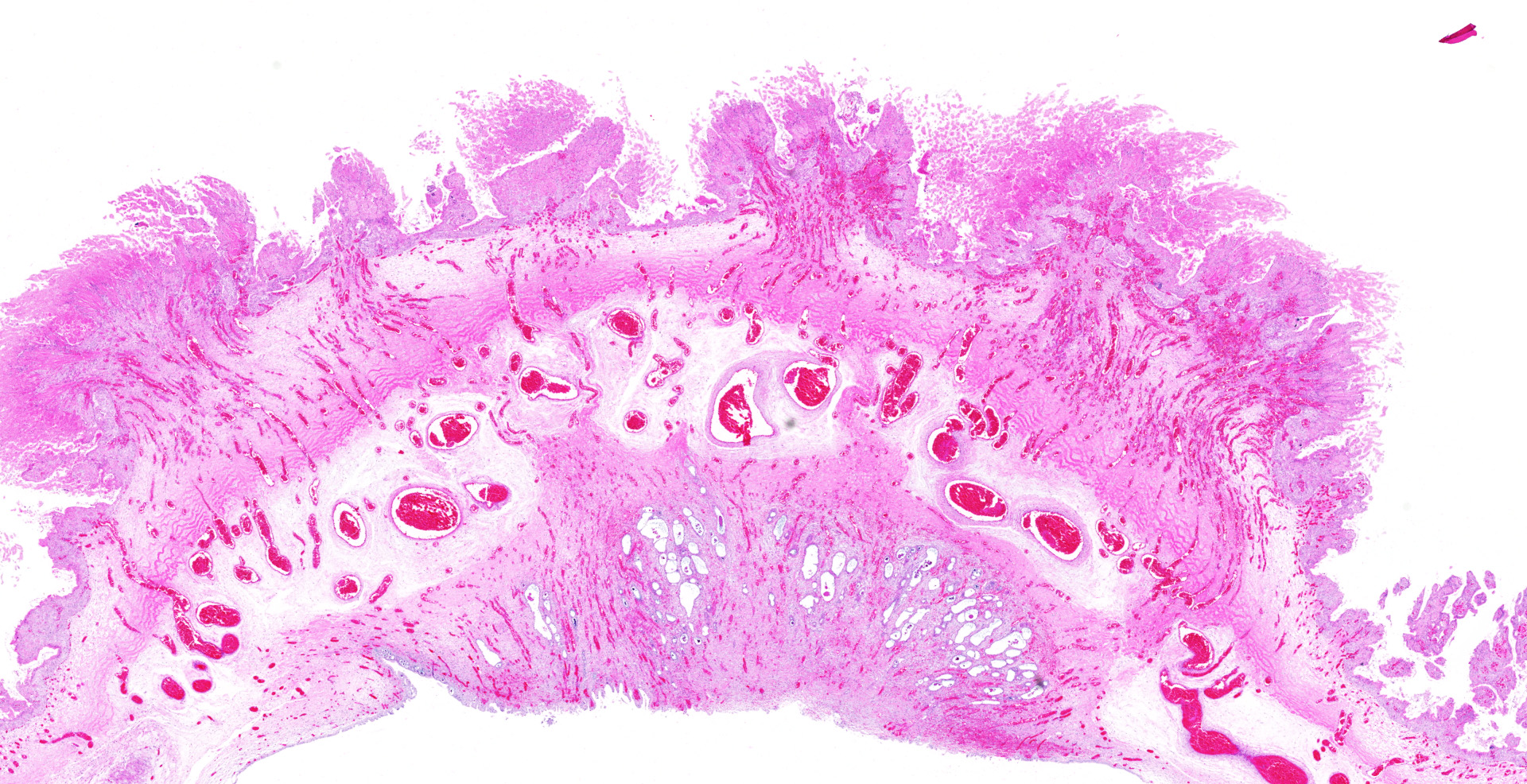
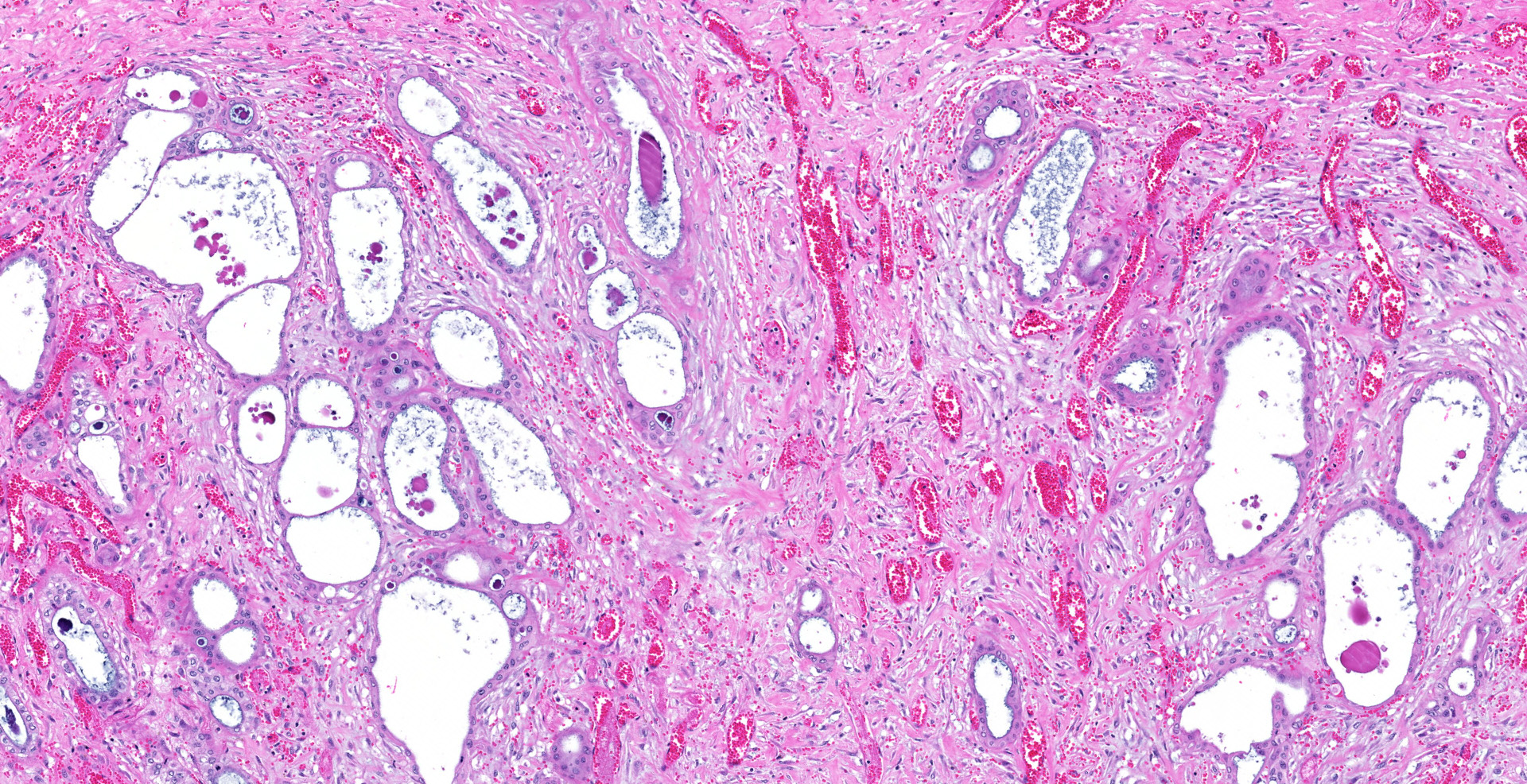
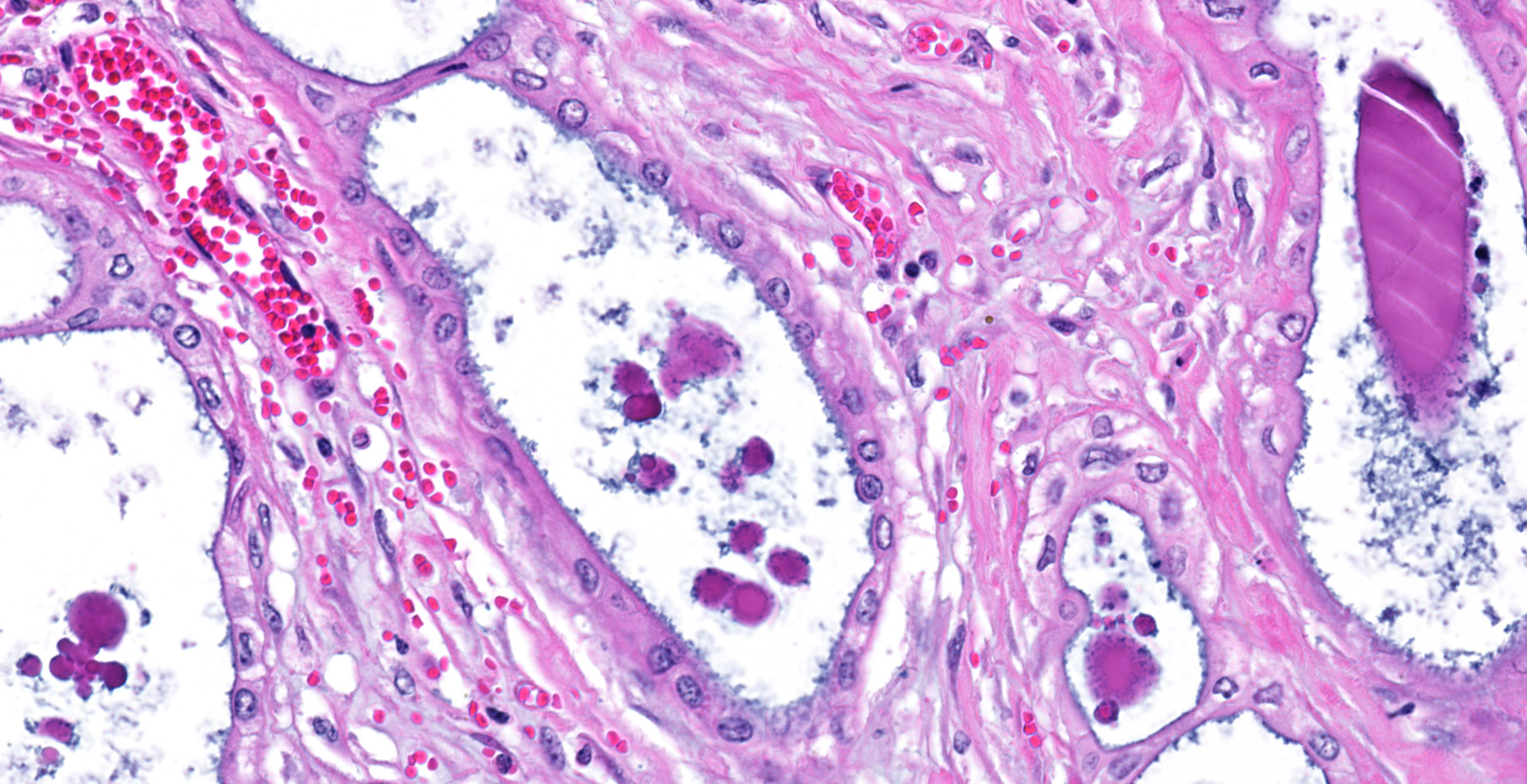
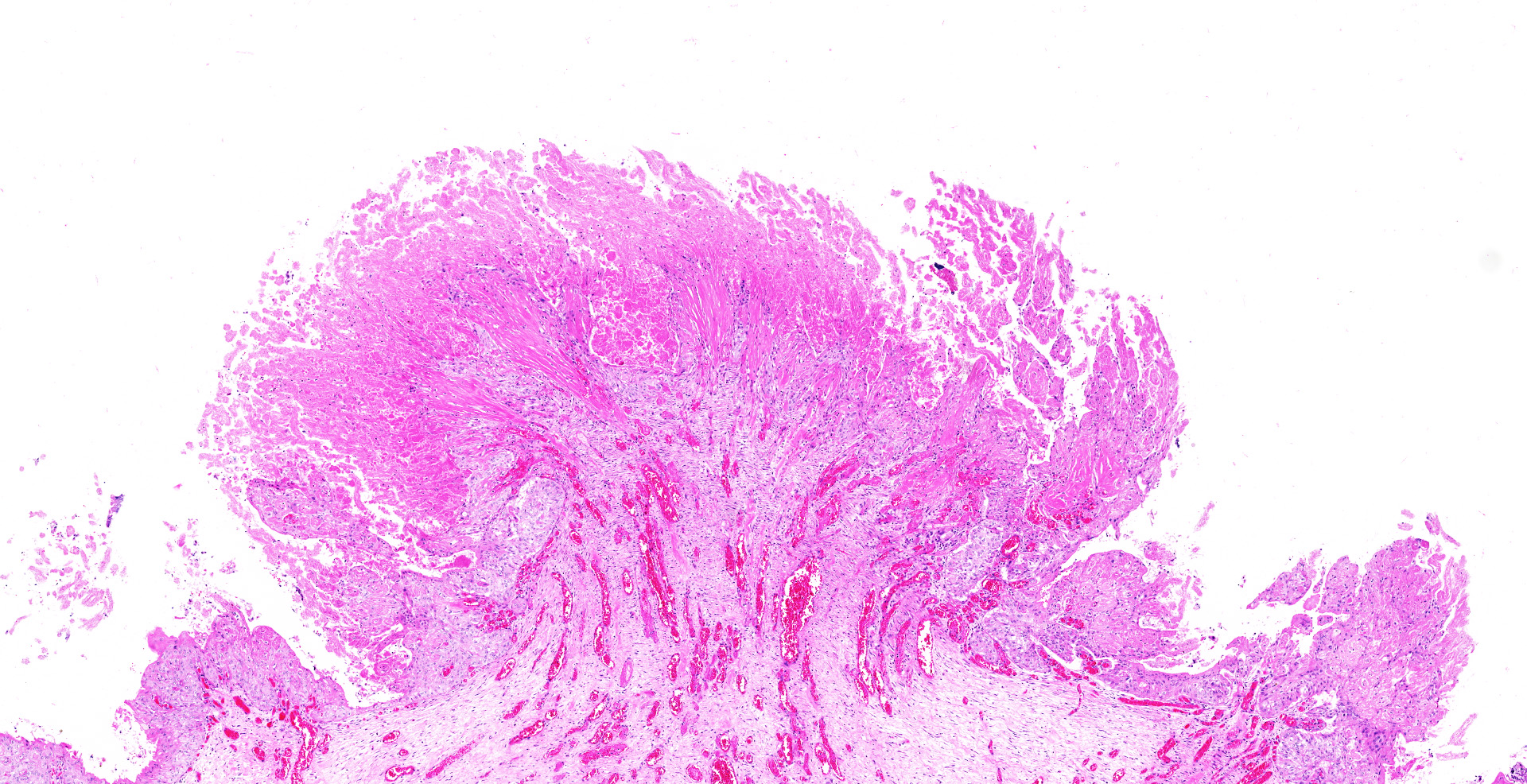
Placenta: A focal area of round epithelial lined structures is present within the fibrous stroma of the chorioallantois that forms a discrete nodule. The allantoic epithelium is stratified with piling of nuclei. Within the epithelium, dilated cystic structures lined by cuboidal epithelium with round nuclei. The cysts are filled with homogenous eosinophilic material. Similar dilated epithelial lined cystic structures are observed within the allantoic stroma of various sizes. Fibrosis, neovascularization and hemorrhage lie between the cysts in the chorioallantoic membrane. Edema is present below the chorionic villi, within the connective tissue. The chorionic villi demonstrate multiple foci of karyorrhexis and pyknotic epithelial nuclei, indicative of necrosis. Several regions of the villi are blunted. Few arteries and arterioles have clear cytoplasmic vacuoles within the tunica media and endothelium, interpreted as hydropic degeneration.
Contributor's morphologic diagnosis:
Marked multifocal to coalescing chronic allantoic epithelial fibroadenomatous hyperplasia with edema and neovascularization. Mild to moderate multifocal acute chorionic villus coagulation necrosis with villus atrophy.
Contributor's comment:
Adenomatous hyperplasia of the allantoic epithelium is categorized in three stages. Stage 1 includes hypertrophic and hyperplastic allantoic epithelium with intraepithelial glands and intracytoplasmic vacuoles. Stage 2 includes the presence of glands within a thickened and reactive allantoic stroma. Stage 3 includes numerous glands of various sizes within the stroma forming a nodule.6 This is a case of stage 3 fibroadenomatous hyperplasia of the allantoic epithelium. Adenomatous hyperplasia has been associated with other chronic placental lesions including nocardia, fungi, Streptococcus spp., Pseudomonas spp., Staphylococcus spp., and coliform (predominately Escherichia coli) placentitis.6 However, these lesions are characterized by focal chorionic villar necrosis, and inflammatory cells within the mass and chorionic epithelium. Acute placentitis has not been associated with adenomatous hyperplasia suggesting that it may be a reactive lesion due to a chronic irritant.6
A study reviewing cases of placental leptospirosis reported 95% of affected placentas demonstrating allantochorionic lesions, the most frequent being adenomatous hyperplasia of allantoic epithelium. Also commonly observed was leukocyte infiltrates within the chorionic villi and stroma, vasculitis, and chorionic villar necrosis, atrophy, and mineralization.7
Contributing Institution:
Department of Veterinary Biosciences
College of Veterinary Medicine
The Ohio State University
http://vet.osu.edu/biosciences
JPC diagnosis:
Placenta, allantois: Hyperplasia, adenomatous, focally extensive, moderate, with fibrosis, neovascularization, and coagulation necrosis of opposing chorionic villi.
JPC comment:
The condition was first reported in 1988 as adenomatous dysplasia of the equine allantois, but similar lesions have been reported near the umbilicus on the allantoic surface of placentas in elephants and rhinoceroses. These lesions have never been reported in other animals or humans.5
Adentomatous hyperplasia or dysplasia of the equine allantois is currently considered by most authors to occur secondary to chronic placental pathology of other causes.1,3,8 The grading scale of lesions, which can be focal or multifocal, was described above. These lesions likely do not directly affect placental function directly. In a case series documenting 8 cases of cystic adenomatous hyperplasia of the allantois, many mares had normal foals prior to an abortion, and at least 3 went on to have subsequent normal foals.8
It is currently not known whether the criteria for the staging occur in a chronologic fashion, or different histologic features manifest independently. The degree, or stage, of disease does not appear to correlate with severity of any symptoms, extent of inflammation, or a particular pathogen.3
While we cannot know the underlying prevalence in the spectrum of healthy births, there is a high prevalence of abortion and bacterial placentitis associated with this condition. Because the histologic changes do not correlate with an acute placentitis, it has been proposed that this condition may predispose the mare to developing a secondary bacterial placentitis.1,3
An important differential for this entity is amnion nodosum, which is characterized by the presence of numerous small papules or granular amorphous nodules on the amnionic surface. A report of amnion nodosum was reported in a Belgian draught horse in 2011 and, similar to many horses affected by adenomatous dysplasia of the allantois, the mare and foal continued to be healthy with no adverse effects noted.2,4
References:
1. Foote AK, Ricketts SW, Whitwell KE. A racing start in life? The hurdles of equine feto-placental pathology. Equine Veterinary Journal. 2012; 44(Suppl. 41):120-129.
2. Govaere J, Vercauteren G, Coopmans C, et al. Amnion nodosum in a Belgian draught horse. Vet Rec. 2011;168(1):22.
3. Hulskotter K, Aurich C, Kohne M, Baumgartner W, Wohlsein P. Die equine adenomatöse Allantoishyperplasie ? ein Warnsignal? Tierarztl Prax Ausg. 2019;47(6):391-396.
4. Lewis SH, Post MD, Benirschke K. Placenta. In: Mills SE ed. Histology for Pathologists, 4th Ed. Philadelphia, PA: Lippincott Williams & Wilkins. 2012:1160-1164.
5. McEntee M, Brown T, McEntee K. Adenomatous dysplasia of the equine allantois. Vet Pathol. 1988:25:387-389.
6. Hong CB, Donahue JM. Adenomatous Hyperplasia of Equine Allantoic Epithelium. Vet Pathol. 1993; 30:171-175.
7. Poonacha KB, Donahue JM. Leptospirosis in Equine Fetuses, Stillborn, and Placentas. Vet Pathol. 1993; 30: 362-369.
8. Shivaprasad HL, Sundberg JP, McEntee K, et al. Cystic adenomatous hyperplasia of the equine allantois: a report of eight cases. J Vet Diagn Invest. 1994;6:107-110.