Signalment:
A 5-year-old spayed female Rhodesian Ridgeback dog (
Canis familiars).The dog was presented for a large (approximately 7 cm diameter), subcutaneous moveable mass over the left shoulder. Two weeks after surgical excision, the dog presented with neurologic signs and blindness. Euthanasia was elected because of poor prognosis.
Gross Description:
There is a 14 cm diameter, fluid-filled, ulcerated subcutaneous mass present over the left shoulder (seroma). The abdominal lymph nodes are enlarged (2x2x2 to 2x3x1.5 cm diameter). On cut section, the architecture of lymph nodes is effaced by white-tan tissue with no clear distinction of cortex and medulla.
Histopathologic Description:
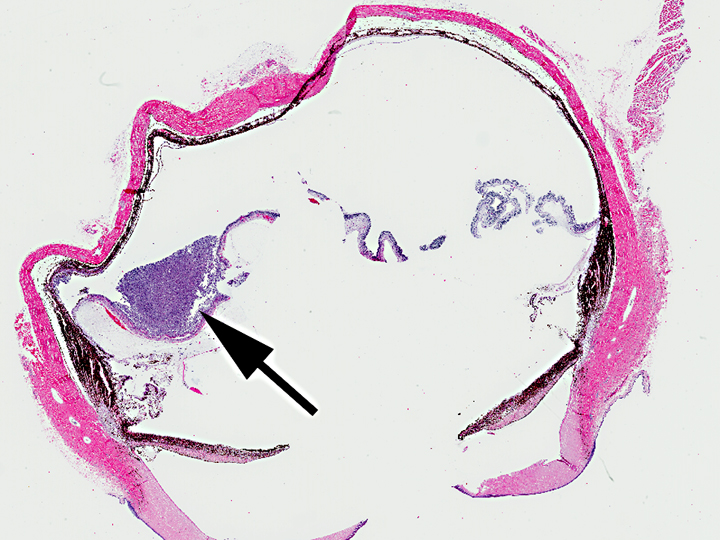
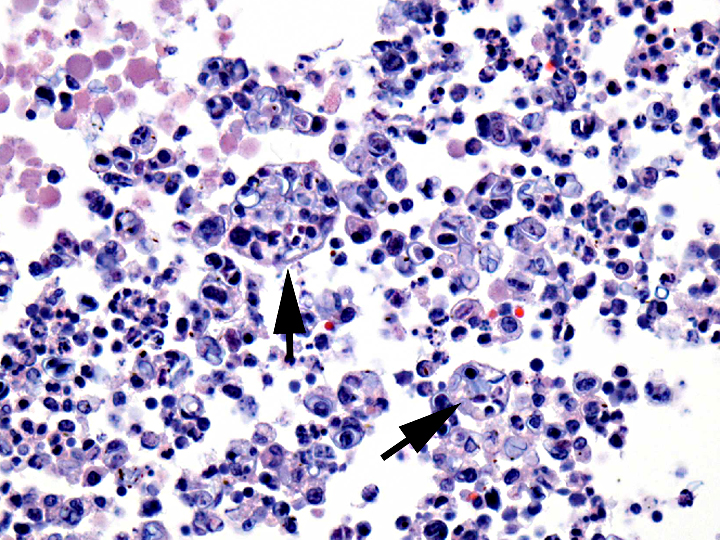
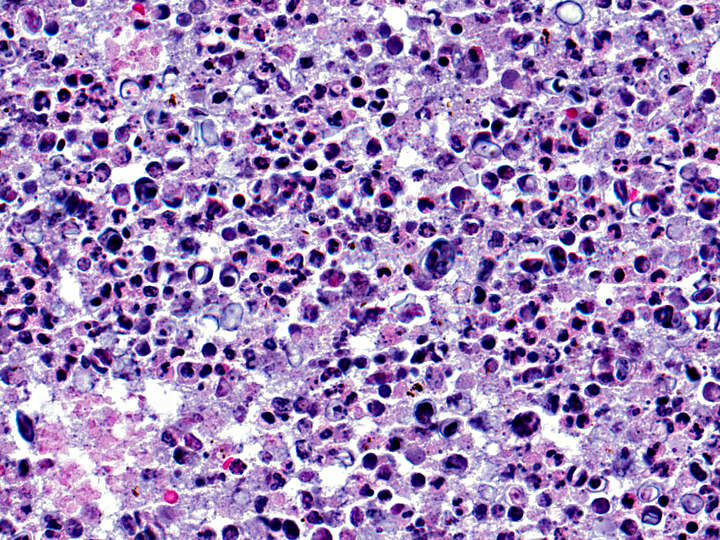
Eye. The subretinal space is diffusely expanded by large numbers of histiocytes, lymphocytes, degenerate and intact neutrophils, mixed with eosiniophilic cellular and karyorrhectic debris, fibrin and numerous extracellular and intrahistiocytic algae. The algae are round to oval, 15-25 microns in diameter, with a 2-3 micron thick cell wall and a basophilic round nucleus. Occasionally, algae contain 2-3 wedge shaped 5-10 micron diameter, round to oval, basophilic endospores. Multifocally, the above-mentioned inflammatory cells extend to the posterior choroid, retina and occlude the trabecular meshwork. A segment of the tapetal retina shows marked hypertrophy (tomb-stoning) of the RPE. The ganglion cells are mostly absent and the inner and outer nuclear layers are attenuated and coalesce. Moderate amounts of eosinophilic fibrillar material (fibrin) are present in the vitreous mixed with few neutrophils, lymphocytes, and plasma cells that adhere to the inner plexiform layer of the retina. Predominantly near the papillary border, the anterior surface of the iris is covered by a single layer of spindle cells (pre-iridal fibrous membrane). The posterior iris epithelium is hyperplastic.
Morphologic Diagnosis:
Eye: Diffuse, severe, granulomatous endophthalmitis with retinal detachment and numerous extracellular and intrahistiocytic algae.
Lab Results:
The cytology smears from the left shoulder mass contain few macrophages and medium sized lymphocytes mixed with small numbers of organisms found both extracellularly and within neutrophils or macrophages. These organisms are reniform to oval and are approximately 15 microns in length and 5 microns in width with a clear capsule. The cytoplasm contains basophilic granules and clear vacuoles without discrete nuclei. The cerebrospinal fluid collected at the time of necropsy shows pleocytosis (nucleated cell count-17,600/microliter) and increased protein levels (516 mg/dL).
Condition:
Prototheca zopfii
Contributor Comment:
The dog had widespread granulomatous inflammation affecting skin, lymph nodes, brain, lung, kidney, ileum, and colon. The histomorphologic features of the algae are consistent with
Prototheca spp. and were confirmed by culture of CSF and urine. Protothecosis is a rare disease caused by
Prototheca spp., a saprophytic achlorophyllous alga affecting a wide range of species.(1) Two pathogenic species of
Protheca has been recognized-
P. zopfi and
P. wickerhamii. The disease has been identified in Europe, Asia, Africa, Australia, islands of the Pacific Ocean, and North America. The organism is ubiquitous and commonly found in raw and treated sewage, slime flux of trees, and animal wastes. Despite the abundance of this organism in nature, the incidence of disease is rare. The disease primarily develops when the hosts immune resistance is suppressed or altered, often by a preexisting or concurrent disease. No preexisting inflammatory, neoplastic or metabolic disease was detected in this dog.
Protothecosis can present either as systemic or localized cutaneous infection. In the alimentary tract,
Prototheca is thought to be an opportunistic invader of existing mucosal lesions. Skin infections are thought to result from traumatic inoculation.(2) In the present case, the dog was initially presented for dermatitis rather than diarrhea and therefore skin was considered to be the primary site of infection in this dog. Cattle, horses, and wild pigs may pass
Prototheca in the feces without apparent clinical disease.
The intestine and the eye are the most common sites in protothecosis of dogs.Â
P. zopfii is almost always isolated from dogs with systemic infections and
P. wickerhamii has been isolated from dogs and cats with cutaneous infections. Grossly, white to tan, 0.2-2 mm diameter, granulomatous lesions can be seen within the affected organs. There is mild inflammation with few macrophages, lymphocytes, plasma cells, and neutrophils mixed with large numbers of algal organisms.(2,3)
Protothecal organisms can be identified on rectal or colonic scrapings if the large intestine is involved.Â
Prototheca sp. are round, oval or angular cells that are 8-20 micron diameter, have a refractile wall and contain granular cytoplasm. The organism reproduces by endosporulation and can be identified histologically as morula of 2-20 daughter cells within a single organism.Â
Prototheca and
Chlorella spp. are morphologically indistinguishable in tissues stained with H&E.Â
Chlorella spp. contain periodic acid-Schiff-positive cytoplasmic starch granules that are PAS-negative following diastase digestion, but
Prototheca spp. do not contain these granules. Ultrastructurally, chloroplasts consist of a highly organized, twisted lamellar component associated with amorphous, electron dense vacuolated material (starch).Â
Prototheca spp. may contain visible starch granules (plastids) on electron microscopy, but these are not associated with a lamellar component.Â
Prototheca organisms must be differentiated from other organisms that undergo endosporulation, such as
Coccidioides immitis and
Rhinosporidium seeberi. Rhinosporidium spp. have large sporangia, filled with uniformly round, 2-10 micron endospores.Â
Coccidioidomyces spp. have spherules that measure up to 50 micron in diameter containing small, round endospores.
Molecular characterization and speciation of the
Protheca spp. can be performed by 18S rDNA sequencing, genotype-specific PCR, restriction fragment length polymorphism, or qPCR followed by DNA Resolution Melting Analysis.(4)
JPC Diagnosis:
Eye: Endopthalmitis, pyogranulomatous, diffuse, severe with numerous algae -- etiology consistent with
Prototheca sp.
Conference Comment:
Ocular protothecosis is only described as part of a systemic infection and never as a primary, solitary lesion. In the eye, it presents as a bilateral granulomatous panuveitis. The primary differential in this case is mycotic endophthalmitis, caused either by
Cryptococcus or
Blastomyces, which produce similar histologic lesions. Conference participants discussed the likely route of infection in this dog being hematogenous, and the necessity of the algae to overcome the blood-ocular barrier via induction of inflammatory cytokines.2 The blood-ocular barrier is composed of the blood-aqueous barrier (which consists of tight junctions in the ciliary body and iridal capillaries and the phagocytic function of the ciliary epithelium) and the blood-retinal barrier (formed by tight junctions in the non-fenestrated capillary endothelium and between the retinal pigment epithelial cells).
References:
1. Greene CE.Â
Infectious Diseases of the Dog and Cat. 3rd ed. St. Louis, MO: Saunders-Elsevier; 2006: 656-662.
2. Wilcock BP. The eye and ear. In: Maxie MG, ed.Â
Jubb, Kennedy, and Palmer's Pathology of Domestic Animals. 5th ed. Vol 1. Philadelphia, PA: Elsevier Saunders; 2007:503-504.
3. Brown CC, et al. Alimentary System. In: Maxie MG, ed.Â
Jubb, Kennedy, and Palmer's Pathology of Domestic Animals. 5th ed. Vol 1. Philadelphia PA, Elsevier Saunders; 2007:231-232.
4. Ricchi M, et al. A rapid real-time PCR/DNA resolution melting method to identify
Prototheca species.
J Appl Micro. 2010;110(1):27-34.Â