Results
AFIP Wednesday Slide Conference - No. 6
13 October 1999
- Conference Moderator:
Dr. Timothy O'Neill, Diplomate, ACVP
Biomedical Research Consultants Inc.
Middletown, MD 21769-6704
-
- NOTE: Click on images for larger views. Use
browser's "Back" button to return to this page.
Return to WSC Case Menu
-
- Case I - 2058 (AFIP 2694987)
-
- Signalment: A four-month-old, female, Suffolk lamb
(Ovis ovis).
-
- History: The lamb was at pasture, doing well, when
she suddenly developed anorexia and ataxia, followed by recumbency.
The lamb died within three days of first showing clinical signs.
The owner gave no treatment. A veterinarian, who was called to
examine the animal shortly before it died, suspected polioencephalomalacia.
Four other lambs in the group were unaffected.
-
- Gross Pathology: There were no significant findings
on the gross necropsy carried out by the practitioner. Fresh
and fixed tissues were submitted for further study.
-
- Laboratory Results:
- Bacteriology: Listeria monocytogenes was cultured
from the brain in heavy growth. Light to heavy growth of E. coli
was cultured from the lung and spleen.
- Toxicology: Kidney and liver samples were negative
for lead and cadmium. Liver analyses for Se, Cu, Zn, Fe, Mn,
were within adequate levels.
Contributor's Diagnosis and Comments: Meningoencephalitis
(brain stem and cerebellum), subacute, severe, mixed cellular
to suppurative, with mononuclear perivascular cuffing, neuropil
edema and microabscessation.
-
- Significant pathological changes in submitted tissues were
limited to the cerebellum and brain stem, notably the medulla.
These are characterized by heavy mononuclear perivascular inflammatory
infiltrates consisting of histiocytes, lymphocytes and plasma
cells; a few neutrophils are also seen. Edema of the affected
areas of the neuropil is prominent and, particularly in sagittal
brain sections, there are multifocally extensive inflammatory
infiltrates with areas of gliosis, microabscessation and focal
neuronal necrosis that extend into the cerebellar corpus medullare.
Depending upon which sections are examined, meninges over affected
brain areas show a variable inflammatory infiltrate, from mild
to focally severe.
In this case, small Gram positive bacilli or coccobacilli resembling
L. monocytogenes were observed most readily within dense
inflammatory cell foci, some of these being microabscesses. The
organisms demonstrated pleomorphism, appearing as small rods
or as coccobacilli. The organisms were seen in small, irregular
clumps or occasionally in short chains and appear to be extracellular.
Less readily defined and stained individual organisms were also
seen within the background that may represent an intracellular,
cytoplasmic, location.
Sagittal and transverse sections of brain are included. Many
of the sagittal sections show extensive lesions. Transverse sections
tend to show affected areas that are more focal or patchy. The
relatively regional area of affected brain tissue within the
brain stem (pons, medulla) and cerebellum emphasizes the importance
of receiving these areas for both culture and for histopathology
from field practitioners seeking a diagnosis. Mild autolysis
is present.
-
- L. monocytogenes is a small Gram positive, facultative
intracellular bacillus that may cause disease in most animal
species, including man (1). Listeriosis in sheep, as in most
other affected species, occurs in 3 distinct syndromes which
seldom overlap (1, 2). These are encephalitis; systemic infections;
and abortion. Less commonly, L. monocytogenes is a cause
of endocarditis and purulent lesions in other organs and tissues
(1). Clinical listeriosis is evidently rare in horses, pigs,
dogs, and cats (3). The organism is ubiquitous in nature and
can be recovered from soil, vegetation, dairy products, animal
feces, and sometimes the oropharynx and tissues of healthy animals
(1, 2, 3).
-
- The disease tends to be seasonal, with clinical cases reported
more commonly in winter or early spring (3); the case reported
here occurred in late May. There is a strong association between
listeriosis and animals fed silage rather than hay. This young
lamb was on pasture grass.
-
- Clinical signs of "circling disease" were not described
in this animal, although it was reported as wobbly or ataxic
prior to recumbency. The pathogenesis of listerial encephalitis
is still only partially understood (2). In the encephalitic form,
the organism is thought to invade the brain via the cranial nerves
(2, 3). Trigeminal neuritis has been reported in 16 of 17 sheep
that were spontaneously affected by listerial encephalitis; the
distribution of lesions in sheep brains also suggested movement
along axon fiber tracts (4). The bulk of evidence is against
the hematogenous route (2). It is not clear how L. monocytogenes
breaches the oral mucosal epithelium, but it has been suggested
that it may penetrate the dental pulp when sheep are cutting
or losing teeth (3). It is interesting that in the ruminant brain
and occasionally in the human brain, the lesions caused by L.
monocytogenes are regionally disseminated small foci of inflammatory
cells, whereas those caused by other pyogenic infections usually
produce one or several large abscesses (4). The organism has
been demonstrated in myelinated axons of the trigeminal nerve
and fiber tracts in the brain stem, and within the cytoplasm
of medullary neurons (2,4); in foci of inflammation it has been
reported as more commonly seen in neutrophils than in macrophages
(4).
The potential for L. monocytogenes to demonstrate pleomorphism
has been well recorded elsewhere, including its ability, in Gram
stains of clinical specimens, to resemble streptococci, to which
it is genetically related (5). Variations in the appearance of
L. monocytogenes grown on culture plates and those identified
in clinical specimens is an interesting point (5), and any comments
by conference participants is welcomed.
-
- Progress has been made in identifying virulence factors in
L. monocytogenes in mice and tissue culture cells, and
presumably these are general principles which influence its virulence
for sheep as well (3). The organism must invade a cell, including
epithelial cells and phagocytes; it multiplies within cell cytoplasm
where, in a poorly understood manner, it appears to be propelled
peripherally. Projections of the infected cell membrane then
invaginate into adjacent cells, and transmit the listeriae. As
a result, L. monocytogenes is able to multiply and spread without
direct exposure to the cells and soluble factors of the extracellular
environment (3).
-
- Listeria monocytogenes is considered a zoonotic agent. Infection
may be transmitted to humans directly from infected meat (e.g.,
hot dogs) or milk, or indirectly from infected cheese made from
unpasteurized milk (2,3).
-
- AFIP Diagnosis: Brain stem and cerebellum: Meningoencephalitis,
subacute, multifocal, moderate, with microabscesses, Suffolk
lamb (Ovis ovis), ovine.
-
- Conference Note: Conference participants agreed with
the contributor's description of the lesions and morphologic
diagnosis. The contributor has provided an excellent review of
listeriosis.
Contributor: Animal Health Centre, 1767 Angus Campbell
Rd, Abbotsford, British Columbia, Canada V3G 2M3.
-
- References:
- 1. Jones CT, Hunt RD, King NW: Veterinary Pathology, 6th
ed, pp. 461-462, Williams and Wilkins, Philadelphia, PA, 1997
- 2. Jubb KVF, Huxtable CR: The nervous System. In: Pathology
of Domestic Animals, 4th ed., vol 1, eds. Jubb KVF, Kennedy PC,
Palmer N. pp. 393-397, Academic Press Inc., NY, 1993
- 3. Czuprynski CJ: Listeria. In: Pathogenesis of Bacterial
Infections in Animals, eds. Gyles CL, Thoen CO, 2nd ed., pp.
70-79, Iowa State Univ Press, Ames, Iowa, 1993
- 4. Charlton KM, Garcia MM: Spontaneous listeric encephalitis
and neuritis in sheep. Light microscopic studies. Vet Pathol
14:297-313, 1977.
5. Mielke MEA, Thomas KH, Unger M: Listeriosis In: Pathology
of Infectious Diseases, vol 1 eds. Connor DH, Chandler FW, Baird
JK, Schwartz DA, Lack EE, Utz JP, pp. 621-633, Appleton &
Lange, Stanford, Connecticut, 1997
-
-
- Case II - B97-8011, 97-14-4 or 97-14-8 or 97-14-9 or 97-15-1
(AFIP 2683969)
-
- Signalment: A four-month-old, male, Hanford-HA minipig
(Sus scrofa domesticus)
-
- History: The sections are from the hearts of two untreated
positive control Hanford minipigs used in a research study to
investigate reperfusion injury following surgical occlusion of
the left anterior descending (LAD) artery. One week prior to
necropsy, the LAD had been occluded for 45-60 minutes followed
by reperfusion, creating a myocardial infarction. As part of
the procedure, the left ventricle and great vessels were instrumented.
Additionally, fluorescent microspheres were injected (peripherally)
during the study period.
-
- Contributor's Diagnoses and Comments:
- 1. Severe sub-acute locally extensive intramural myocardial
infarction with granulation tissue.
- 2. Mild to moderate sub-acute diffuse reactive visceral pericarditis.
- 3. Intravascular microspheres (not present in all sections).
-
- Most sections provided are full thickness through the left
ventricular free wall. The most prominent lesion is locally extensive
intramural sub-acute myocardial infarction, characterized by
complete loss of myocardial tissue with replacement by granulation
tissue. In some sections, islands of myocardium are present within
the damaged region. The interface between infarcted and intact
tissue is usually abrupt, but there are some examples of an infiltrating
pattern. The amount of edema associated with the granulation
tissue varies among the sections. Neutrophils are present, both
free in the granulation tissue and marginated in smaller blood
vessels. Degenerating tissue, characterized by nuclear debris
(karyorrhexis), is scattered throughout the affected tissue.
-
- Generally, the subendocardial and subepicardial regions contain
relatively intact cardiac muscle but some myocardial tissue contains
rarefied, vacuolated cytoplasm. Intact Purkinje fibers are present
in some sections. The visceral pericardium is mildly to severely
reactive, typified by granulation tissue with a variety of inflammatory
cells, predominately neutrophils. Multinucleate giant cells are
present in a few sections. Some sections lack the pericardial
surface. Microspheres (15-17µ in diameter) are present
within small vessels in intact myocardium in many sections.
-
- AFIP Diagnosis: Heart, left ventricle: Cardiomyocyte
loss, focally extensive, with granulation tissue, multifocal
mild lymphocytic, histiocytic and neutrophilic inflammation and
focal chronic proliferative pericarditis (infarct), Hanford-HA
minipig, porcine.
-
- Conference Note: The differential diagnosis discussed
in conference included ischemic injury, vitamin E/ selenium deficiency,
and viral infection. However, the discrete loss of myofibers
with replacement by granulation tissue and mild inflammation
were considered to be most consistent with a subacute to chronic
ischemic insult (infarct).
-
- Ischemia and reperfusion both damage cardiomyocytes. The
severity of injury from infarction is directly related to the
duration of occlusion, location of occlusion and metabolic needs
of the myocardium. Ischemia results in depletion of ATP (within
seconds), loss of contractility (<2 minutes), irreversible
cell injury (20-40 minutes), and microvascular injury (>1
hour). Reperfusion can salvage sublethally damaged cardiomyocytes,
but can also lead to further injury. Reperfusion increases the
generation of oxygen free radicals, supporting the release of
cytokines from damaged cells and the recruitment of inflammatory
cells that cause further injury.
-
- Histologic staging of infarction follows a distinct pattern
based on the time after injury. First signs of coagulation necrosis
occur between 4 and 12 hours. Within 1-3 days, there is continued
coagulation necrosis, loss of cross striation and infiltration
of the interstitium by neutrophils. From days 3-7, there is degeneration
of neutrophils and disintegration of myofibers with peripheral
phagocytosis by macrophages. After 7-10 days, there is well-developed
phagocytosis and formation of granulation tissue.
After two weeks, there is a gradual decrease in cellularity and
deposition of collagen, eventually resulting in a dense scar.
Based on these characteristics, the histologic features present
in this case are in close agreement with the clinical history
of a one-week-old ischemic injury.
-
- Contributor: The Procter & Gamble Company, Miami
Valley Laboratories, PO Box 398707, Cincinnati, Ohio.
-
- Reference:
- Schoen FJ: The Heart. In: The Pathologic Basis of Disease,
eds. Cotran RS, Kumar V, Collins T, 6th ed., pp. 550-563. WB
Saunders Company, Philadelphia, PA, 1999
-
-
- Case III - A41177 (AFIP 2694681)
-
- Signalment: Six-month-old pig (breed and sex unknown).
-
- History: This pig was presented for slaughter at a
federally inspected establishment. The pig was not identified
as abnormal during antemortem inspection.
-
- Gross Pathology: There was hepatomegaly and splenomegaly
with accumulation of yellow material with a lipid-like texture.
The lungs and parietal pleura were discolored (yellow) and there
was a mottled appearance of cut surfaces of thoracic and lumbar
lymph nodes. Mesenteric lymph nodes were enlarged and cut surfaces
were homogenously yellow-orange with a soft texture. The jejunal
mucosa contained yellow plaques. Adipose tissue in skeletal muscle
and heart appeared normal.
-
- Contributor's Diagnoses and Comments:
- 1. Lymph node, Spleen, Liver, Lung: Histiocytosis, diffuse,
marked, with intrahistiocytic vacuoles.
2. Liver: Hepatocellular lipidosis, diffuse, marked.
3. Jejunum: Histiocytosis, diffuse, marked with Touton-type giant
cells, foam cell thrombi, and atheromatous plaques.
Frozen sections revealed that vacuoles in macrophages and hepatocytes
contained lipid. Special stains for bacteria and fungi revealed
no etiologic agents. One possible etiology for these lesions
would be hyperlipidemia secondary to an inherited defect in lipid
metabolism, perhaps combined with a high fat diet. Inbred swine
are a key animal model for study of human familial hypercholesterolemia,
but lesions of this severity are not generally seen in 6- month-old
animals.
-
- Another consideration would be an inherited lipid storage
disease. Two lysosomal storage diseases have been suggested to
occur in pigs. There is a well-defined GM2 gangliosidosis of
Yorkshire pigs that results in primarily neuronal storage. There
also is a single report of a less well-defined disease thought
to be similar to glucocerebrosidosis in which there was vacuolization
of cells in the liver, spleen, and in other visceral organs.
-
- AFIP Diagnoses:
- 1. Small intestine: Histiocytosis, diffuse, severe, with
lipid-type cytoplasmic vacuolation, histiocytic lymphatic emboli
and Touton giant cells, breed unknown, porcine.
2. Spleen: Histiocytosis, multifocal, moderate, with lipid-type
cytoplasmic vacuolation, and multifocal reticuloendothelial cell
hyperplasia.
3. Lung: Histiocytosis, interstitial, diffuse, moderate, with
lipid-type cytoplasmic vacuolation, histiocytic lymphatic emboli
and mild subacute interstitial pneumonia.
4. Liver: Histiocytosis, centrilobular, bridging, portal, and
sinusoidal, mild to moderate with lipid-type vacuolation, and
mild to moderate diffuse lipid-type hepatocellular cytoplasmic
vacuolation.
5. Lymph node: Histiocytosis, diffuse, severe, with lipid-type
cytoplasmic vacuolation and scattered eosinophils.
-
- Conference Note: The conference participants essentially
agreed with the contributor's diagnosis. Differential diagnosis
discussed in conference included fungal infections, mycobacteriosis,
storage diseases (ceroid-lipofuscinosis and GM2 gangliosidosis)
and hypercholesterolemia/ hyperlipemia. Clinical history, blood
lipid profile, knowledge of the breed and diet, evaluation of
related pigs, and electron microscopy could provide additional
information to help differentiate storage diseases from hypercholesterolemia/hyperlipemia.
-
- Contributor: USDA FSIS OPHS Eastern Laboratory, PO
Box 6085, Russell Research Center, 950 College Station Road,
Athens, GA, 30604
-
- References:
- 1. Attie AD: The spontaneously hypercholesterolemic pig as
an animal model for human atherosclerosis. ILAR News 30:5-12,
1988
- 2. Jolly RD, Walkley SU: Lysosomal storage diseases of animals:
an essay in comparative pathology. Vet Pathol 34:527-548, 1997
- 3. Kosanke SD, Pierce KR, Bay WW: Clinical and biochemical
abnormalities in porcine GM2 gangliosidosis. Vet Pathol 15:685-699,
1978
- 4. Kosanke SD, Pierce KR, Read WK: Morphogenesis of light
and electron microscopic lesions in porcine GM2 gangliosidosis.
Vet Pathol 16:6-17, 1979
- 5. Pierce, KR, Kosanke SD, Bay WW, Bridges CH: GM2 Gangliosidosis,
Model No. 104. In: Handbook: Animal Models of Human Disease,
Fasc. 6, Eds. TC Jones, DB Hackel, G Migaki. Registry of Comparative
Pathology, AFIP Washington, DC, 1977
- 6. Sandison AT, Anderson LJ: Histiocytosis in two pigs and
a cow: conditions resembling lipid storage disorders in man.
J Pathol 100:207-210, 1970
-
-
- Case IV - 96-636 (AFIP 2694731)
-
- Signalment: One-year-old, breed not specified, male
guinea pig (Carva cobaya)
-
- History: Found dead in an animal nursery.
-
- Gross Pathology: Consolidation of all pulmonary lobes,
marked splenic hyperplasia, moderate lipidosis of the liver,
multiple hemorrhages of the mucous membranes of stomach, colon
and rectum.
-
- Laboratory Results: Lung: E. coli, Klebsiella oxytoca,
Pasteurella haemolytica, Lactobaccillus sp., Moraxella sp.
Contributor's Diagnoses and Comments:
- 1. Lung: pneumonia, interstitial, diffuse, severe with numerous
macrophages within the alveolar lumina and basophilic intranuclear
inclusion bodies.
- 2. Lung vessels: perivascular edema, severe, acute thrombosis
of small vessels and basophilic intranuclear inclusion bodies
in endothelial cells.
- 3. (Not submitted) Liver: moderate lipidosis, basophilic
intranuclear inclusion bodies in hepatocytes and endothelial
cells.
- 4. Spleen: basophilic intranuclear inclusion bodies in unidentified
cells.
-
- Etiology: consistent with adenovirus infection.
-
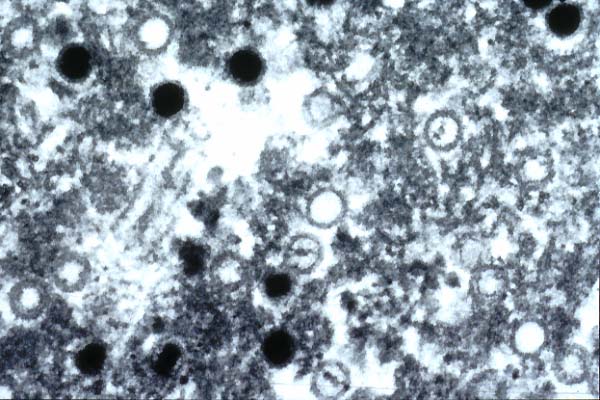
- The diagnosis of adenovirus-infection was established by
electron-miroscopic investigation. Within the nuclei of hepatic
endothelial cells, numerous round virus particles were identified.
They measure approximately 90nm in diameter and some have an
electron-dense core while others have an electron-lucent core.
The size and appearance of the viral particles are characteristic
for adenovirus. The first reports on a spontaneous respiratory
disease in guinea pigs caused by adenovirus (Namann et al., 1981;
Brennecke et al., 1983) gave reason for an experimental proof
of the infection (Kaup et al., 1984; Kunsty et al., 1984).
- Case 6-4. Note multiple electron dense viral particles
and other immature membrane bound particles which contain developing
central nucleoids.
-
- The case presented was observed 2 years after a first case
of adenovirus-infection in a guinea pig, equally examined by
EM. Unfortunately, culture of the virus was not attempted; hence
it is not feasible to confirm the diagnosis. With regard to the
literature cited, there is not much doubt about the nature of
the virus. Both cases are described in detail in the article
cited in the references below.
-
- AFIP Diagnosis: Lung: Pneumonia, interstitial, subacute,
diffuse, moderate, with multifocal fibrin thrombi and intrahistiocytic
and endothelial basophilic and eosinophilic intranuclear inclusion
bodies, guinea pig (Carva cobaya), rodent.
-
- Conference Note: Although pneumonia is a common cause
of death in guinea pigs, the cause is usually bacterial. Common
etiologic agents include Bordetella bronchiseptica, Streptococcus
pneumoniae, Streptococcus zooepidemicus, Klebsiella pneumoniae,
and Pasteurella multocida. Relatively common causes of viral
infections in guinea pigs include cytomegalovirus, lymphocytic
choriomeningitis virus and a few enteric viruses. Adenoviral
pneumonia was diagnosed and experimentally reproduced in the
early 1980's but has been reported rarely. Adenoviruses cause
natural respiratory disease in cattle, sheep, horses, quail,
nonhuman primates, dogs, and man, and experimental disease in
swine and mice.
-
- Differential diagnosis considered for this case included
cytomegalovirus and adenovirus. Both of these viruses produce
a similar histologic appearance, with large intranuclear inclusions.
Cytomegalovirus causes prominent cytomegaly and by electron microscopy,
there are 100-150 nm diameter, hexagonal viral nucleocapsids
within nuclei of infected cells. Electron microscopy of adenovirus
infected cells demonstrates 70-90 nm virions that are sometimes
arranged in paracrystaline arrays.
The bar in the submitted electronmicrograph equals 100nm. The
size and morphology of the viral particles are consistent with
an adenovirus. An immunohistochemical stain for adenovirus performed
at the AFIP was positive.
-
- Contributor: Institute of Veterinary Pathology, Veterinaerstr.
13, 80539 Muenchen, Germany.
-
- References:
- 1. Brennecke C H, Dreier TM, Stokes WS: Naturally occurring
virus-associated respiratory disease in two guinea pigs. Vet
Pathol 20:488-491, 1983
- 2. Breuer W, Haunichen T, Hermanns W: Adenovirus-induced
pneumonia in two guinea pigs. Berl Munch Tieruerztl Wschr, 110:51-53,
1997
- 3. Feldman SH, Richardson JA, and Clubb FJ, Jr: Necrotizing
viral bronchopneumonia in guinea pigs. Lab Anim Sci 40:82-83,
1990.
4. Harris IE, and Goydich W: Adenoviral bronchopneumonia of guinea
pigs. Aust Vet J 62:317, 1985
- 5. Kaup FJ, Naumann S, Kaup FJ, Kraft V, Knocke KW: Adenovirus
pneumonia in guinea pigs: an experimental reproduction of the
disease. Lab Anim 18:55-60, 1984
- 6. Kunstyr I, Maess J, Naumann S, Kaup FJ, Kraft V, and Knocke
KW: Adenovirus pneumonia in guinea pigs: an experimental reproduction
of the disease. Lab Anim 18:55-60, 1984
- 7. Naumann S, Kunstyr I, Langer I, Maess J, Hoerning R: Lethal
pneumonia in guinea pigs associated with a virus. Lab Anim 15:235-242,
1981
-
- J Scot Estep, DVM
Captain, VC, USA
Registry of Veterinary Pathology*
Department of Veterinary Pathology
Armed Forces Institute of Pathology
(202)782-2615; DSN: 662-2615
Internet: estep@afip.osd.mil
-
- * The American Veterinary Medical Association and the American
College of Veterinary Pathologists are co-sponsors of the Registry
of Veterinary Pathology. The C.L. Davis Foundation also provides
substantial support for the Registry.
-
- Return to WSC Case Menu