Results
AFIP Wednesday Slide Conference - No. 20
- February 10, 1999
-
- Conference Moderator:
Dr. Steven E. Weisbrode, Diplomate, ACVP
The Ohio State University
Department of Veterinary Biosciences
- Columbus, OH 43210
-
- NOTE: Click on images for larger views. Use
browser's "Back" button to return to this page.
Return to WSC Case Menu
-
Case I - N1893 (AFIP 2420927)
- Signalment: Two-month-old, female, Blonde d'Aquitane
calf.
-
- History: The calf presented with severe lameness,
swelling of the interphalangeal joints, and gangrene of the left
forelimb and hindlimb. The calf had received treatment for pneumonia
and septicemia at seven days of age. Lameness was first noted
at five weeks of age.
-
- Gross Pathology: The limb extremities were variably
swollen with localized hair loss, ulceration, and sloughing of
the hooves. Bony sequestra in the distal metacarpus and distal
metatarsus of the left forelimb and hindlimb were sharply defined.
Fibrinopurulent exudate was present in the interphalangeal joints
of both forelimbs.
 A
A B
B C
C
- Case 20-1.Gross Images. The limbs in (A) demonstrate
variable amounts of dry gangrene affecting only the hoof, hoof
and toe, or hoof, toe, & metatarsal region of the leg. Note
the sequestrum in the distal metatarsal bone of (C).
-
- Laboratory Results: Salmonella dublin was isolated
from the joint exudate and colon.
-
- Contributor's Diagnosis and Comments: Terminal dry
gangrene; Osteomyelitis and arthritis.
-
- Etiology: Salmonella dublin.
-
- Microscopically, necrosis and fibrinopurulent debris
are prominent at the level of the distal growth plate of the
metacarpal bone. Mature and fragmented neutrophils are common,
fibrin thrombi are present in small blood vessels, and there
is widespread necrosis of cartilaginous, osseous, and myeloid
elements. Lesions extend into the epiphysis and diaphysis, and
occasional clefts are present in the growth plate cartilage.
The necrotic areas are poorly circumscribed by mononuclear leukocytes
and dense fibrovascular stroma. Microscopic findings in other
tissues included histiocytic foci (paratyphoid nodules) in the
liver and crypt abscesses in the ileum.
-
- Hematogenous osteomyelitis in calves frequently involves
the growth plates of long bones and vertebral bodies. The increased
susceptibility of metaphyseal bone has been related to local
features of small blood vessels that favor localization of circulating
bacteria, leading to thrombosis and necrosis. These features
include loop formations, endothelial gaps, sluggish circulation,
and lack of anastomoses.
-
- Most cases of hematogenous osteomyelitis in calves result
form infection with either Salmonella dublin or Arcanobacteria
(Actinomyces) pyogenes. Advanced cases of Salmonella dublin infection
sometimes progress to terminal dry gangrene. The gangrenous appearance
of the extremities has been compared with that seen in ergot
poisoning in this species. Records of previous illness, including
diarrhea and septicemia, in affected calves and other problems
associated with salmonellosis in affected herds are not unusual.
 4x
obj
4x
obj 10x
obj
10x
obj
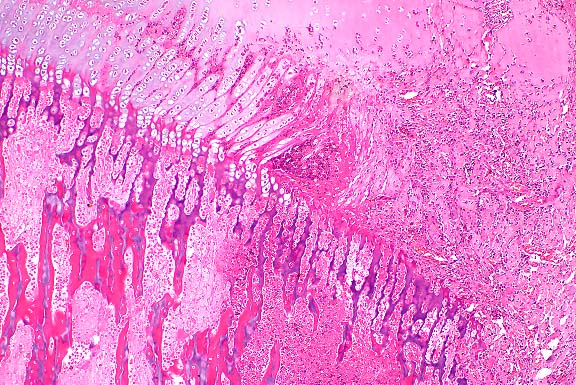
- Case 20-1. Bone. At the margin of the necrotic sequestra
(left), which extends through the growth plate, there is a mixture
of degenerate neutrophils, fibrin, edema, and cell debris (right).
 10x
obj
10x
obj
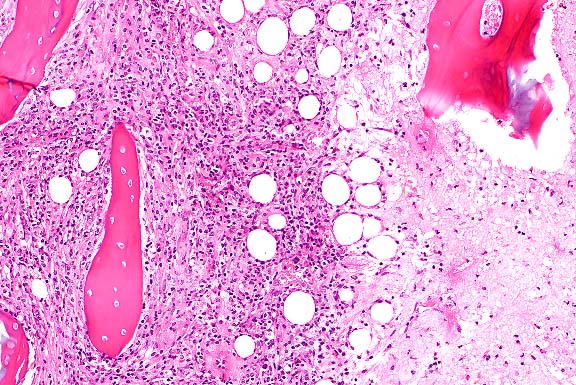
- Case 20-1. Bone. The necrotic bone (right), and marrow
is being replaced by neutrophils, macrophages and fibroblasts
forming collagen (center & left).
- AFIP Diagnosis: Bone: Necrosis, coagulative, focally
extensive (infarct), with moderate multifocal chronic-suppurative
osteomyelitis and physitis, and fibrosis, Blonde d'Aquitane,
bovine.
-
- Conference Note: Depending on the sections examined,
conference participants identified many of the histologic features
described by the contributor. Multifocally, the physeal cartilage
is characterized by hypereosinophilia of the matrix, chondrocyte
nuclear pyknosis, karyolysis, and loss (necrosis), with scattered
fissures. Within some sections, variable numbers of viable and
degenerate neutrophils, lymphocytes, and macrophages have infiltrated
and disrupted the physeal cartilage and the spicules of woven
bone within the primary spongiosa. Immature fibrous connective
tissue, similar inflammatory cells and variable amounts of cellular
debris have replaced the growth plate and primary spongiosa.
In other sections, the predominant findings are extensive coagulative
necrosis of cartilage and primary spongiosa bounded by zones
of granulation tissue and small numbers of inflammatory cells.
-
- Within the epiphysis of most sections, trabecular bone is
frequently hypereosinophilic, and there is karyolysis and loss
of osteocytes (necrosis). Occasionally, viable woven bone is
found deposited upon spicules of necrotic trabecular bone, and
diffusely there are increased amounts of mesenchymal tissue with
scattered inflammatory infiltrates and cellular debris similar
to that in the physis.
-
- Based on the histologic findings of extensive coagulative
necrosis of cartilage and bone with surrounding fibrosis, several
conference participants favored an ischemic etiology, such as
ergotism, over an infectious agent. Several participants had
difficulty distinguishing inflammation from bone marrow myeloid
elements, and did not identify a major inflammatory component
within the lesion. In the submitted gross photos, a cross-section
of one of the limbs demonstrates necrosis and lysis of bone,
and the inflammatory process extends outward into the skin. The
gross findings and the microscopic pattern of inflammation and
necrosis suggest an embolic bacterial etiology rather than an
ischemic process, such as that found in ergotism. Those sections
dominated by coagulative necrosis and extensive fibrosis may
reflect the histologic appearance of "dry gangrene"
discussed by the contributor in association with Salmonella infections
of bone.
-
- Bacterial osteomyelitis develops either by direct implantation
into the affected bone, as may occur in trauma, or as a result
of hematogenous infection. Hematogenous infections occur most
frequently in neonates or juvenile animals and children. In children
and animals, the most frequent sites of inoculation are areas
characterized by rapid growth and increased risk of trauma, such
as the growth plates located at the proximal and distal aspects
of long bones.
-
- The microvascular anatomy of the metaphysis is unique; large
caliber veins with little collateral circulation are present,
which leads to marked slowing of blood flow and increased susceptibility
to thrombosis and colonization by hematogenous bacteria. Thrombosis
and venostasis of the metaphysis seem to be important in the
development of osteomyelitis in adult humans, and are most frequently
associated with trauma.
-
- Salmonellosis may lead to thrombosis as a result of endotoxemia.
Bacterial lipopolysaccharide induces vascular dilatation, pooling
of blood, activation of platelets and leukocytes, complement
fixation, and release of vasoactive amines, leading to thrombosis.
Thrombi in metaphyseal vessels serve as foci for bacterial implantation
in septicemic animals, with subsequent development of osteomyelitis.
An acute, neutrophilic inflammatory response follows bacterial
implantation, with production of fibrin and exudate. Continued
exudation and inflammation cause increased tissue pressures due
to edema. The inelastic nature of bone complicates and exacerbates
the increases in tissue pressure, resulting in greatly decreased
blood flow to the affected area, ischemia, and necrosis of bone
and cartilage. This mechanism probably explains the findings
of dry gangrene and coagulative necrosis in bacterial osteomyelitis.
Extensive osteonecrosis interferes with the penetration of antibiotics
and frequently complicates the treatment of bacterial osteomyelitis.
-
- Contributor: Department of Veterinary Pathology, Faculty
of Veterinary Medicine, University College Dublin, Shelbourne
Road, Ballsbridge, Dublin 4, Ireland.
-
- References:
- 1. Firth EC, Kersjes AW, Dik KJ, Hagens FM: Haematogenous
osteomyelitis in cattle. Vet Record 120:148-152, 1987.
- 2. Morgan JP, Van De Watering CC, Kersjes AW: Salmonella
bone infection in colts and calves: Its radiographic diagnosis.
J Amer Vet Radiol Soc 15:66-76, 1974.
- 3. O'Connor PJ, Rogers PAM, Collins JD, McErlean BA: On the
association between salmonellosis and the occurrence of osteomyelitis
and terminal dry gangrene in calves. Vet Record 91:459-460, 1972.
- 4. Palmer N: Bones and joints. In: Pathology of Domestic
Animals, Jubb KVF, Kennedy PC, Palmer N, eds., 4th edition, vol.
1, pp. 101-109, Academic Press, San Diego, CA, 1993.
- 5. Bullough PG: Bone and joint infection. In: Bullough and
Vigorita's Orthopaedic Pathology, 3rd edition, pp. 107-121, Mosby-Wolfe,
London, England, 1997.
-
Case II - 980264-5 (AFIP 2641219)
- Signalment: One-year-old, male, European cat.
-
- History: The cat was referred to the Department of
Medicine at the Ecole Nationale Vétérinaire d'Alfort
because it had developed numerous firm growths over the right
and left scapulae, the right ribs, and the pelvis beginning at
six months of age. The animal was anorectic and thin, and it
had locomotion problems. A radiograph confirmed the clinical
examination, and after several days, the animal developed a low
and irregular femoral pulse. Vessel compression was excluded
as the cause of the pulse irregularities, and the cat was electively
euthanized.
-
- Gross Pathology: At necropsy, many masses were observed.
On the left and right scapulae, we observed three masses of almost
8 cm in diameter with irregular margins. The masses were heterogeneous
in color, being white on the periphery and red-gray in the middle.
The masses were coalescing and hard. On the right ribs, we observed
only one mass, which measured 8 cm in diameter and involved the
three first ribs of the right hemithorax. We could see the remnant
of one rib in the center of the mass. The other aspects of this
mass were similar to the first one. On the pelvis, we noted a
single mass on the right ileum measuring 4 cm in diameter that
compressed the pelvic vessels. This mass was heterogeneous in
color with a hemorrhagic center.

- Case 20-2. Gross images. This composite photo illustrates
the external, surface, and cross-sectional views of the multinodular
growth of cartilage-covered bone typical of this disease which,
in this cat, affected the ribs, both scapulae, and pelvis.
-
- Laboratory Results: None.
-
- Contributor's Diagnosis and Comments: Feline osteochondromatosis.
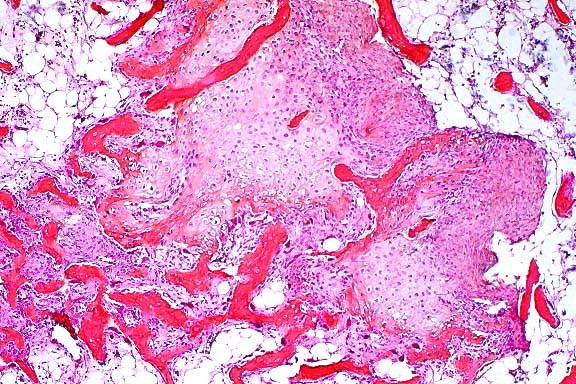
- Microscopic examination revealed a tumor-like mesenchymal
proliferation consisting of chondrocytes forming a rim of hyaline
cartilage surrounding spongy bone. The cortex of each growth
was irregular, and the spongy bone had trabeculae supporting
fatty marrow. Remnants of cartilage persisted in the osseous
mass. The histological picture suggests a peripheral chondromatous
proliferation followed by imperfect central endochondral ossification.
-
- Osteochondroma is an abnormal cartilaginous growth with endochondral
ossification. The term osteochondromatosis indicates that there
are multiple lesions. This disease is reported in dogs, cats
and horses. There is no sex or breed predilection, but it is
consistently observed in adult animals. According to Pool (6),
feline osteochondromas usually have a biphasic pattern, with
a cover of cartilage giving rise to a bony base by endochondral
ossification.
-
- In man, the origin of osteochondromatosis is probably hereditary
or congenital. Particles resembling feline leukemia virus and
transmissible feline sarcoma virus have often been detected in
the lesions found in cats with osteochondromatosis; their etiologic
significance remains unclear.
 4x
obj
4x
obj
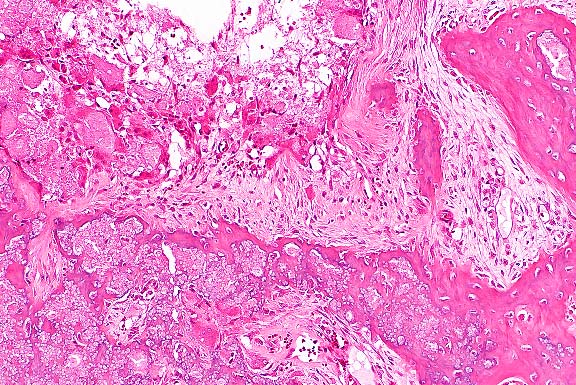
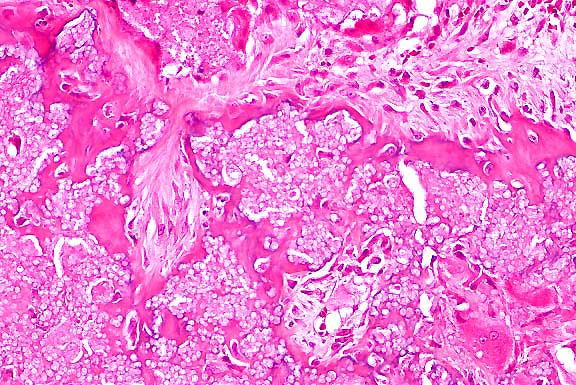
- Case 20-2. Bone. Irregular endochondral bone formation
occuring deep within cancellous bone. Dark cells in the lower
right are osteoclasts.
-
- AFIP Diagnosis: Scapula: Osteochondromatosis, Domestic
Shorthair, feline.
-
- Conference Note: Osteochondromas are cartilage-capped,
partially ossified protuberances or exostoses that are usually
multicentric, but may occur singly. The condition occurs in cats,
horses, dogs, and humans. The disease in dogs and horses differs
from that in cats in clinical presentation, skeletal distribution
and proposed cause. The condition in dogs, horses, and humans
is inherited as an autosomal dominant trait. Tumors occur on
the long bones of young animals, are thought to arise from dysplastic
or ectopic growth plates, often become progressively larger as
the animal matures, and cease to grow at skeletal maturity. Tumors
do not occur on bones of intramembranous origin, such as the
skull or scapula. Usually, the lesions in dogs and horses are
of little clinical significance unless there is mechanical interference,
although malignant transformation to chondrosarcoma or osteosarcoma
may occur in long standing lesions of adult animals.
-
- In contrast to dogs and horses, tumors in cats arise after
skeletal maturity, are distributed randomly throughout the skeletal
system including intramembranous bone (e.g. the skull), demonstrate
progressive growth similar to a neoplasm, and proliferating cells
located at the surface of lesions may contain viral particles
that resemble feline leukemia virus and feline sarcoma virus.
The tumors are thought to arise from periosteal mesenchymal cells
in lesions of intramembranous bone. Malignant transformation
of benign lesions and appearance of new lesions may occur in
cats, heralding a grave prognosis.
-
- Histologically, osteochondromas of dogs and horses recapitulate
the zones of development found in the normal epiphyseal growth
plate. Microscopic examination reveals a variably thick cartilage
cap with scattered areas of mineralization covered by a thin
layer of fibrous periosteum. The cap of hyaline cartilage is
bordered at the base by regularly arranged cancellous bone which
is produced by orderly endochondral ossification in actively
growing lesions. Trabeculae of cancellous bone are separated
by marrow elements. In old lesions in adult animals, extensive
endochondral ossification may result in little or no cartilage
remaining at the apical surface. Feline osteochondromatosis differs
microscopically from the inherited condition in young dogs and
horses in that the cartilage is irregular, chondrocytes are haphazardly
arranged, endochondral ossification is less orderly, and the
hyperplastic periosteum may directly form bone.
-
- Contributor: Ecole Vétérinaire d'Alfort,
Laboratoire d'Anatomie Pathologique
7, Avenue du Général de Gaulle, 94704 Maisons Alfort,
France.
References:
- 1. Newell MS, Roberts RE, Baskett A: Presumptive tenosynovial
osteochondromatosis in a horse. Vet Radio Ultras 37:112-115,
1996.
- 2. Pool RR, Carrig CB: Multiple cartilaginous exostoses in
a cat. Vet Pathol 9:350-359, 1972.
- 3. Magnussen KL: What is your diagnosis? (Osteochondromatosis
in a cat). J Amer Vet Med Assoc 210:1733-1734, 1997.
- 4. Hubler M, Johnson KA, Burling RT, Francis DF, Ratcliffe
CC: Lesions resembling osteochondromatosis in two cats. J Small
Anim Pract 27:181-187, 1986.
- 5. Doige CE: Multiples osteochondromas with evidence of malignant
transformation in a cat. Vet Pathol 24:457-459, 1987.
- 6. Pool RR: Tumors of bone and cartilage. In: Tumors in domestic
Animals, Moulton JE, ed., 3rd ed., pp. 168-172, Univer. of California
Press, Berkeley, 1990.
- 7. Brown RJ, Trevethan WP, Henry VL: Multiple osteochondroma
in a Siamese cat. J Amer Vet Med Assoc 160:433-435, 1972.
- 8. Jones TC, Hunt RD, King NW: Skeletal system. In: Veterinary
Pathology, 6th ed., pp. 841-842, Williams and Wilkins, Baltimore,
1997.
- 9. Palmer N: Diseases of bones. In: Pathology of Domestic
Animals, Jubb KVF, Kennedy PC, Palmer N, eds., 4th ed., vol.
1, pp. 129-130, Academic Press, San Diego, CA, 1993.
- 10. Bullough PG: Cartilage-forming tumors and tumor-like
conditions. In: Bullough & Vigorita's Orthopaedic Pathology,
3rd ed., pp. 107-121, Mosby-Wolfe, London, 1997.
- 11. Slayter MV, et al.: Bone and Joint Tumors. In: World
Health Organization International Histological Classification
of Tumors in Domestic Animals, 2nd Series, vol. 1, pp. 6, 22-24,
Armed Forces Institute of Pathology, Washington DC, 1994.
-
Case III - A44016 (AFIP 2638315)
- Signalment: 18-month-old, female, ostrich (Struthio
camelus).
-
- History: The ostrich was presented for slaughter at
a Texas slaughter facility. No antemortem abnormalities were
noted at the slaughter facility. No other clinical history is
available.
-
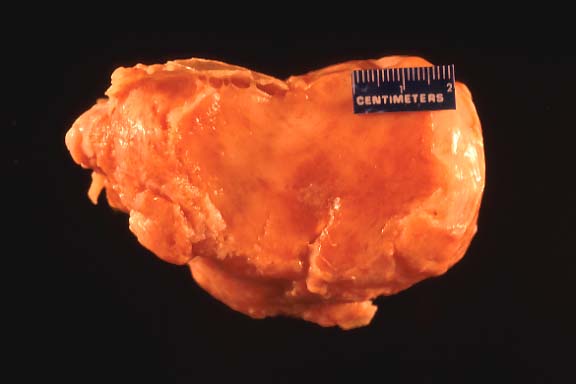
- Gross Pathology: Per the submitting inspection veterinarian:
"suspicious mass, 15 cm long by 8-9 cm wide, in the right
pelvic area arising from the right iliac wing; mass appeared
balloon-shaped with bony deposition on the caudal end, and a
large soft tissue growth with a thin bony covering on the cranial
end. The mass was attached to the ventral surface of the vertebral
column in three areas by firm bony attachments." The frozen
tissue, submitted on request, had central white to tan somewhat
fibrous soft tissue with irregular lightly reddened areas dispersed
throughout. There was a thin, white, irregular bony capsule (1-3
mm thick).

- Case 20-3. Gross Image
-
- Laboratory Results: Several immunohistochemical studies
were performed on sections of the mass.
1. Muscle specific actin and vimentin antibodies did not work
on ostrich control muscle.
2. Smooth muscle actin was negative in ostrich tumor tissue,
except for smooth muscle around scattered vessels.
3. Cytokeratin, neuron specific enolase, and S-100 protein were
negative in tumor tissue.
-
- Contributor's Diagnosis and Comments: Giant cell reparative
granuloma of bone (iliac and subvertebral, young ostrich, female).
-
- Iliac, subvertebral mass: There is a dense fibrous capsule
of some section borders which contains individualized and flattened
bone multifocally. There is abundant, moderately cellular stroma
with flattened to plump spindle cells and abundant mature collagen.
Multifocally, there is a lightly basophilic matrix that stains
with alcian blue for mucopolysaccharide. Scattered foci of more
dense homogenous eosinophilic stroma with embedded nuclei are
noted. There are discrete islands of multinucleate giant cells
that have approximately 6 to up to 30 nuclei, and abundant eosinophilic
cytoplasm. These cells surround and are occasionally found within
small non-muscular vessels. The cytoplasm occasionally contains
iron positive hemosiderin material, or has small cleft-like vacuoles.
These latter cells often have light blue staining of the cytoplasm
with alcian blue. The vessels are variably congested, with some
small foci of hemorrhage and a few hemosiderophages. Trichrome
staining reveals abundant collagen throughout, positive staining
in more homogenous stromal areas, and occasionally centrally
around multinucleate giant cells.
-
- The lesion, as grossly described and as examined histologically,
is most consistent with a giant cell reparative granuloma of
bone. The islands of giant cells associated with and within vessels
with an abundant stroma and collagenous and mucopolysaccharide
rich matrix differentiate this from a giant cell tumor. In giant
cell tumor, the giant cells are more dispersed, there is less
matrix, and the stroma is usually mononuclear in type with some
spindle cells and significant mitotic activity. The difficulty
of finding antibodies which work in this species, and the inavailability
of some specialized antibodies, precluded any further immunohistochemical
staining of the lesion at this time. Further examination of this
lesion is to be performed for publication of this lesion in an
ostrich (unreported as to my knowledge).
 4x
obj
4x
obj 10x
obj
10x
obj
 40x
obj
40x
obj
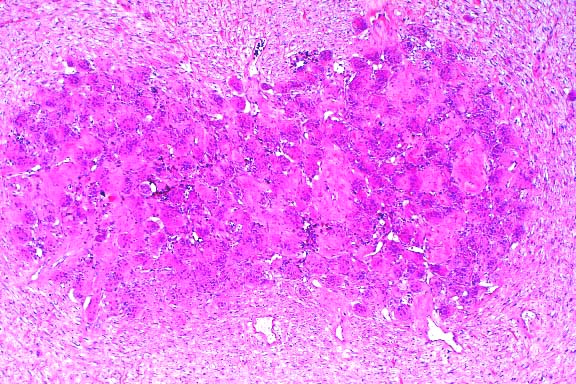
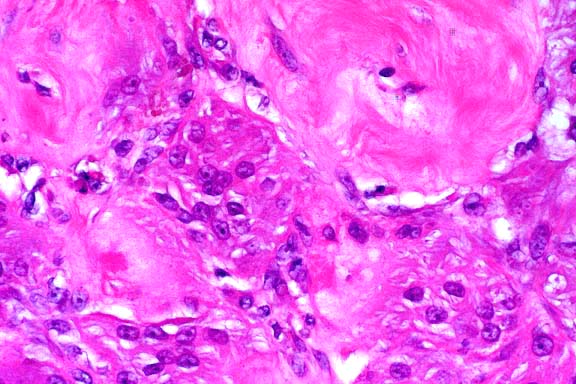
- Case 20-3. Tumor. Normal bone is replaced by streams
& bundles of spindle cells and multifocal clusters of multinucleate
giant cells.
- AFIP Diagnosis: Bone (right iliac wing, per contributor):
Fibroma, with numerous osteoclast-like giant cells, ostrich (Struthio
camelus ), avian.
-
- Conference Note: Conference participants were divided
on the interpretation of the microscopic findings and the nature
of the lesion in the bone of this ostrich. Like the contributor,
some participants interpreted the mass as a reactive fibrous
lesion with scattered clusters of multinucleated giant cells
and spicules of mineralized lamellar bone. Other attendees identified
a neoplasm of fibrous tissue composed of spindled cells arranged
in haphazard streams and bundles with aggregates of large multinucleate
giant cells within a dense collagenous matrix. Multinucleate
cells contain up to 30 nuclei and have vacuolated cytoplasm.
Rare mitoses were noted within the spindled cell population.
At the natural margins of some sections, the spindled cells extended
through and multifocally effaced the preexistent cortex. In some
areas, small amounts of hemorrhage and hemosiderin are found
in association with the giant cells. Inflammatory cells are absent.
-
- Members of the Department of Orthopedic Pathology interpreted
the lesion as a neoplasm within the fibroma "family."
The growth characteristics of the tumor, with an expanding shell
of bone and low mitotic activity, suggest an indolent lesion.
Scattered aggregates of osteoclast-like giant cells are found
in some human fibromas, but they are not as numerous as in this
case. The orthopedic pathologists considered the giant cells
an intrinsic component of the neoplastic process rather than
a secondary reactive phenomenon. Differential diagnosis for similar
lesions in humans would include osteoclastic fibroma and variant
fibromyxoma (both of which are oral, head, or neck lesions),
and an unusual desmoplastic fibroma.
-
- Human giant cell reparative granulomas (GCRG) represent reactive,
non-neoplastic lesions thought to occur as the result of intraosseous
or subperiosteal hemorrhage. While the lesion in this ostrich
does share some microscopic features with human GCRG, such as
the presence of hemorrhage and hemosiderin within nodular clusters
of multinucleated giant cells in abundant fibroblastic tissue,
GCRG does not extend through the cortex of the affected bone.
Additionally, there is no zonal orientation of the lesion in
the ostrich that would suggest a reactive process.
-
- Contributor: United States Dept. of Agriculture, FSIS,
OPHS, Pathology Russell Research Center, College Station Road,
P.O. Box 6085, Athens, Georgia 30604.
-
- References:
- 1. Fechner RE, Mills SE: Tumors of the bones and joints.
In: Atlas of tumor pathology, 3rd series, Fascicle 8, pp.173-186,
Armed Forces Institute of Pathology, Washington DC, 1993.
- 2 . Trigo FJ, Leathers CW, Brobst DF: A comparison of the
canine giant cell tumor and giant cell reparative granuloma of
bone. Vet Pathol 20:215-222, 1983.
- 3. Ung F, Kasey K, Keith D, McKenna MJ: Giant cell reparative
granuloma of the temporal bone: Case report and review of the
literature. Otolaryngol Head Neck Surg 118:525-529, 1998.
- 4. Kenan S, Lewis MM, Abdelwahab IF, Klein M: Subperiosteal
giant cell granuloma. J Bone Joint Surg 76:810-813, 1994.
- 5. Bullough PG: Benign non-matrix producing bone tumors.
In: Bullough & Vigorita's Orthopaedic Pathology, 3rd ed.,
pp. 405 , Mosby-Wolfe, London, 1997.
-
Case IV - 98-1975 (AFIP 2641612)
- Signalment: Canine, German Shepherd Dog, male, seven
months of age.
-
- History: The dog had lameness of the right foreleg
of two weeks duration. A firm to hard, 4 x 6 cm mass was palpated
and removed. The mass appeared to be adjacent to a cervical vertebral
process on the right side. Two days post surgery, the dog was
no longer lame.
-
- Gross Pathology and Laboratory Results: None described.
-
- Contributor's Diagnosis and Comments: Fascia adjacent
to cervical vertebrae: Calcinosis circumscripta (tumoral calcinosis),
chronic, with chondro-osseous metaplasia.
-
- The lesions of tumoral calcinosis and calcinosis circumscripta
have been reported in dogs, horses, monkeys, man, and recently
also in cattle and cats. Sites of occurrence in the dog include
cutaneous or periarticular locations in footpads, bony prominences
of limbs, cervical vertebral region, tongue, cheek, and pinna.
Cervical juxtavertebral lesions have occasionally been associated
with compression of the spinal cord and ataxia. An intramedullary
case and a lesion involving synovial tissue have been reported.
Large dogs account for about 90% of canine tumoral calcinosis
cases, with German shepherd dog being most commonly affected.
-
- With rare exceptions, tumoral calcinosis lesions appear grossly
as hard, spherical, nonpainful, subcutaneous or periarticular
swellings which are often large and encapsulated, and which usually
exude a granular, gritty, white, paste-like material on cut surface.
Early lesions appear histologically as multifocal subcutaneous
accumulations of amorphous lightly basophilic material which
is periodic acid-Schiff positive, stains brown with acid orcein
Giemsa, and can be shown by von Kossa stain to contain calcium.
Within the basophilic material, hemorrhage is occasionally seen,
and fractures or fissures are seen commonly, but inflammatory
and fibroplastic responses are negligible. Intermediate lesions
are more likely to have fully mineralized areas within the amorphous
material, which is surrounded by mild to moderate granulomatous
inflammation and fibroplasia. Late lesions are associated with
marked granulomatous inflammation and fibroplasia, with macrophages,
multinucleate giant cells, lymphocytes, and a few plasma cells
and neutrophils. Inflammatory cells are arranged around mineralized
centers in palisading granuloma fashion. Although these centers
are generally acellular, they do incorporate some macrophages,
fibroblasts, and histiocytic giant cells containing phagocytized
mineral. Granulomatous areas are separated by thick connective
tissue septa. Cartilaginous or osseous metaplasia is seen in
56.9% of late lesions. Very old lesions are multilocular, with
thick connective tissue trabeculae, and are characterized by
completely mineralized areas without much active inflammation.
-
- Several possible etiologies for tumoral calcinosis have been
proposed. These include: repetitive trauma with dystrophic mineralization;
cystic dilation, hyperplasia, and mineralization of apocrine
glands; collagen vascular disease; and local or systemic metabolic
disorders. In humans, normophosphatemic periarticular tumoral
calcinosis is strongly associated with previous trauma. In dogs,
renal failure is associated with footpad lesions. In hyperphosphatemic
tumoral calcinosis patients without renal insufficiency, there
may be an inherited proximal tubular defect that causes excessive
tubular reabsorption of phosphorus.
 10x
obj
10x
obj
 20x
obj
20x
obj 20x
obj
20x
obj
- Case 20-4. Cervical vertebra. Multifocally areas of
endochondral bone partly replaced by granular mineralized debris
are surounded by macrophages, foreign body giant cells, and fibrous
connective tissue.
-
- AFIP Diagnosis: Cervical vertebral fascia (per contributor):
Granulomas, calcareous (calcinosis circumscripta), with fibrosis
and chondro-osseous metaplasia, German Shepherd Dog, canine.
-
- Conference Note: In most cases, canine calcinosis
circumscripta probably represents dystrophic calcification, since
it occurs in sites that are often affected by trauma or in which
trauma is known to have occurred, such as ears that have been
cropped. The reason young, large breed dogs are predisposed is
undetermined, but their active calcium and phosphorus metabolism
may be involved.
-
- In humans, tumoral calcinosis is reported most frequently
in individuals of African descent, especially during the first
two decades of life. The disease presents as large, firm, irregularly
shaped, mineralized masses, usually located in the vicinity of
large joints such as the hip, lateral shoulder, and posterior
elbow. The lesions are usually asymptomatic and only rarely cause
discomfort. Occasionally, ulceration of the overlying skin with
secondary bacterial infection and fistula formation occurs.
-
- Contributor: Department of Veterinary Biosciences,
The Ohio State University, 1925 Coffey Road, Columbus, OH 43210.
References:
- 1. Lewis DG, Kelly DF: Calcinosis circumscripta in dogs as
a cause of spinal ataxia. J Small Anim Pract 31:36-38, 1990.
- 2. Marks SL, Bellah JR, Wells M: Resolution of quadriparesis
caused by cervical tumoral calcinosis in a dog. J Amer Anim Hosp
Assoc 27:72-76, 1991.
- 3. Scott DW, Buerger RG: Idiopathic calcinosis circumscripta
in the dog: A
retrospective analysis of 130 cases. J Amer Anim Hosp Assoc 24:651-658,
1988.
- 4. Smack DP, Norton SA, Fitzpatrick JE: Proposal for a pathogenesis-based
classification of tumoral calcinosis. Intern J Dermatol 35:265-271,
1996.
- 5. Jones TC, Hunt RD, King NW: The skin and its appendages.
In: Veterinary Pathology, 6th ed., pp. 849-850, Williams and
Wilkins, Baltimore, MD, 1997.
- Conference Coordinator:
- Ed Stevens, DVM
Captain, United States Army
Registry of Veterinary Pathology*
Department of Veterinary Pathology
Armed Forces Institute of Pathology
(202)782-2615; DSN: 662-2615
Internet: STEVENSE@afip.osd.mil
-
- * The American Veterinary Medical Association and the American
College of Veterinary Pathologists are co-sponsors of the Registry
of Veterinary Pathology. The C.L. Davis Foundation also provides
substantial support for the Registry
- Return to WSC Case Menu
 A
A B
B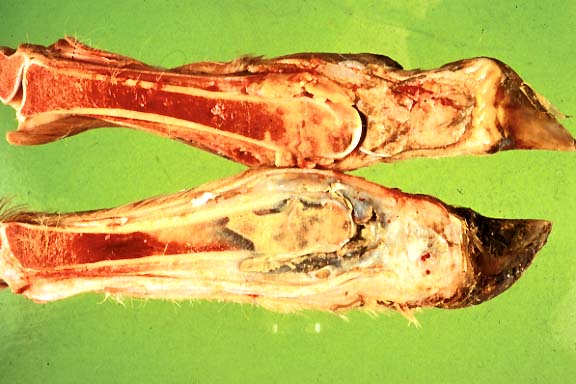 C
C
 4x
obj
4x
obj 10x
obj
10x
obj
 10x
obj
10x
obj

 4x
obj
4x
obj
 4x
obj
4x
obj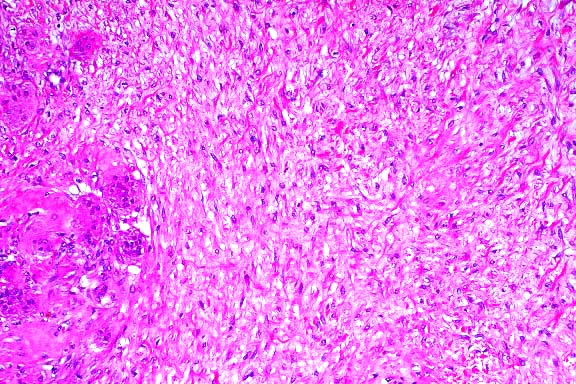 10x
obj
10x
obj
 40x
obj
40x
obj
 10x
obj
10x
obj
 20x
obj
20x
obj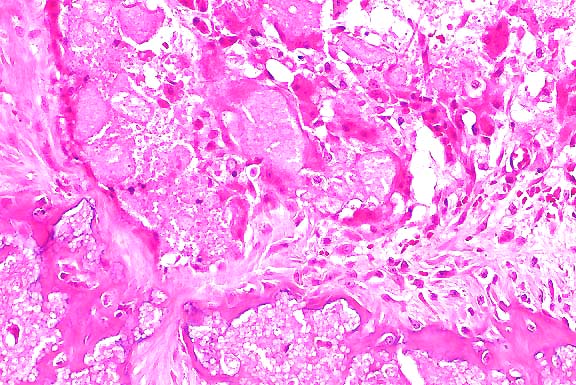 20x
obj
20x
obj